Pros and Cons of Dietary Strategies Popular Among Cancer Patients
This article discusses some of the popular diets that cancer patients pursue, and the positive and negative aspects associated with these diets.


Oncology (Williston Park). 32(11):542-7


Suzanna Maria Zick, ND, MPH



Detrick Snyder, MPH


Donald I. Abrams, MD

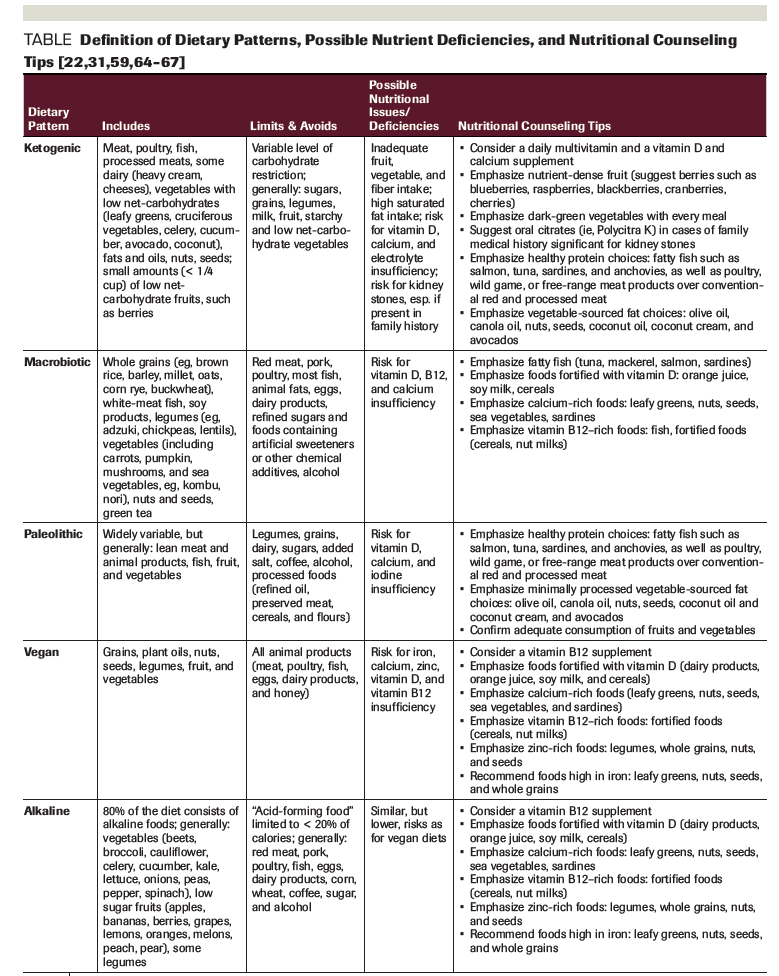
Table. Definition of Dietary Patterns, Possible Nutrient Deficiencies, and Nutritional Counseling Tips
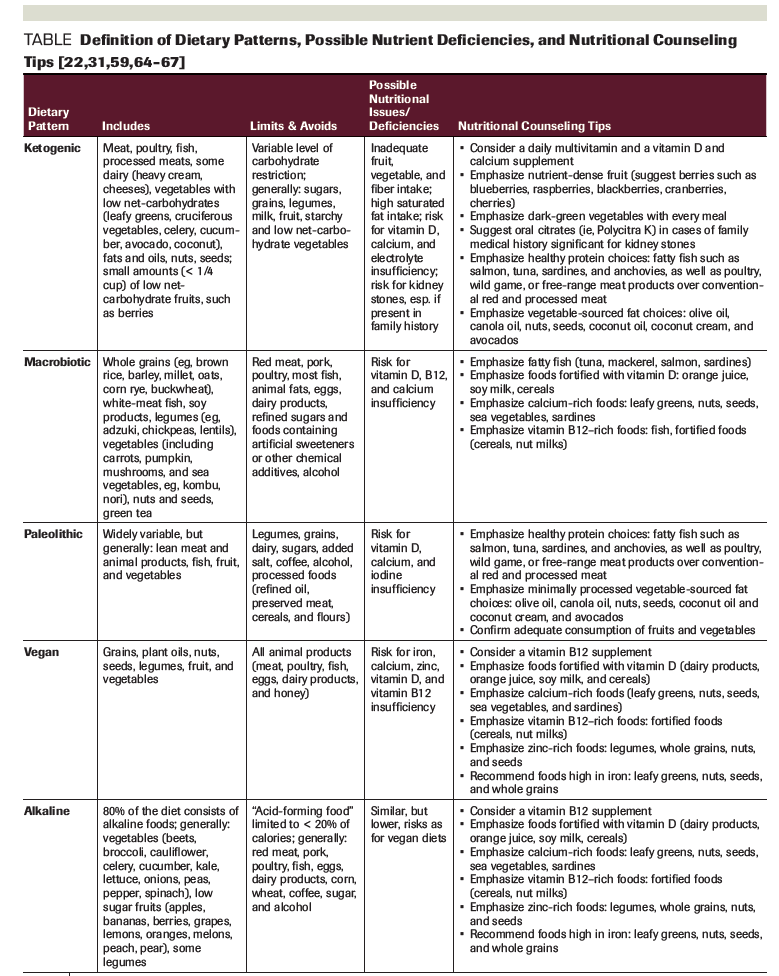

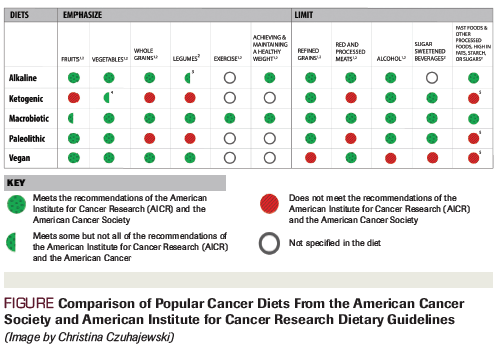
Figure. Comparison of Popular Cancer Diets From the American Cancer Society and American Institute for Cancer Research Dietary Guidelines
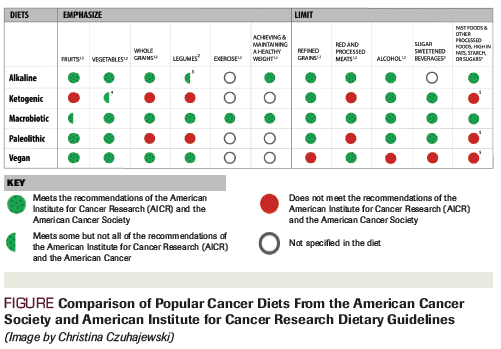
As many as 48% of cancer patients pursue popular diets, including the alkaline, Paleolithic, ketogenic, vegan, and macrobiotic diets, with the hope that they will improve survival and prevent recurrence. These diets have positive aspects consistent with the dietary guidelines proposed by the American Cancer Society (ACS) and the American Institute for Cancer Research (AICR). All of the diets emphasize eating vegetables, all but the ketogenic diet encourage eating fruit, and all but the vegan diet limit refined grains and alcohol. Both the macrobiotic and the alkaline diets meet the majority of the ACS and AICR guidelines. Negative aspects of these diets include pseudo-scientific rationales for their anti-cancer properties, limited evidence that they improve cancer outcomes, the possibility for nutrient insufficiencies, and elimination of food groups proven beneficial for cancer prevention and general health. Moreover, with nutritional counseling, nutrient insufficiencies and misalignment with cancer clinical guidelines can often be addressed. Clinicians should consider strategies to encourage evidence-based dietary changes that encourage positive features of popular cancer diets, while minimizing negative aspects.
Introduction
There is considerable interest in making lifestyle changes, including dietary changes, among cancer patients and survivors.[1] Both the American Cancer Society (ACS)[2] and the American Institute for Cancer Research/World Cancer Research Fund (AICR/WCRF)[3] have clinical dietary guidelines specific to cancer patients. These guidelines are evidence-based reviews of dietary intake on decreasing the risk of, and mortality from, cancer. Numerous large prospective epidemiological studies have shown that a high level of adherence to the ACS and AICR dietary guidelines significantly decreases the incidence of cancer, from 17% to over 50%, depending on cancer site, and decreases cancer-specific mortality by 20% to 30%.[4-8]
Cancer patients and survivors, however, rarely use dietary guidelines to inform their dietary choices. Instead, surveys among cancer patients and survivors have indicated that “special diets,” such as vegan and macrobiotic diets, are among the most commonly used integrative therapies, with as many as 48% of cancer patients or those at increased risk of cancer adopting these diets.[9-14] In contrast to the ACS and AICR nutrition guidelines, there is limited research on the impact of these popular diets on cancer-specific outcomes, such as incidence, mortality, and quality of life. This leaves clinicians with scarce information on how to advise their cancer patients on the use of these diets.
The purpose of this review is to help oncology providers gain knowledge about the content, rationale, and science of the diets that are popular among cancer patients. Specifically, we examine five of these popular diets: the alkaline, Paleolithic, ketogenic, vegan, and macrobiotic diets, using three different frameworks. The first framework is a series of three questions proposed by nutritionist Marion Nestle about how to evaluate any diet. These three questions are: 1) “What is it?” 2) “Is the rationale behind it logical?” and 3) “Does it promote health?”[15] The second framework is to determine what, if any, scientific evidence supports these popular diets for cancer patients, and the third framework is to determine to what extent these special diets concur with the ACS and AICR clinical dietary guidelines.
Alkaline Diet
Proponents of the alkaline diet believe that most cancers are caused by an acidic environment in the body and that the primary cause of this presumed acidosis is acid-forming foods (see Table).[16] The Western diet is characterized by high intake of animal products and refined carbohydrates, with limited consumption of fruit and vegetables, and is thus considered to be highly acid-forming. In contrast, the alkaline diet, designed to provide more alkaline ions after digestion, is rich in fruits and vegetables, with limited protein; it decreases acid load; and it helps to reduce strain on acid-detoxification systems.[17,18] Proponents assume that it will raise systemic pH and that its effects can be assessed by monitoring urine pH. Indeed, a clinical trial in healthy adults comparing an alkaline diet vs an acidic one found that, when urine pH increased by 1.02 units, systemic pH had a significant increase of 0.014 units, indicating that urine pH may be a valid indicator of systemic pH.[19]
Fang Fang Zhang, MDAssociate Professor, Tufts University Friedman School of Nutrition Science and Policy, Boston, MassachusettsClinicians Need to Play a Larger Role in Advising Cancer Patients on NutritionDespite prolonging their life spans, cancer survivors have a substantially reduced quality of life due to symptoms from both malignancies and their treatments, and they are at an elevated risk of premature mortality and serious morbidity. Clear evidence supports the benefits of optimal nutrition in this population, which range from relieving symptoms and treatment-related side effects to improving survival and quality of life. However, cancer survivors’ nutritional intake remains inadequate: their adherence to the Dietary Guidelines for Americans is poor, and their intake patterns are worse when compared with the general population.[1]While many cancer patients and survivors are highly motivated to seek information about dietary changes to improve their long-term health, nutrition care is largely lacking in the current delivery model of outpatient oncology.[2] In the United States, about 70% of cancer survivors reported that they had never received nutrition advice from their providers.[3] As a result, they often seek nutrition information on the internet, or adopt a popular dietary strategy-such as the alkaline, Paleolithic, ketogenic, or vegan diet-that is not supported by strong scientific evidence.Cancer patients and survivors report a strong desire to receive nutrition advice from their healthcare providers. The gap between such an aspiration for improved health and their poor dietary intake highlights the need for adequate nutrition support for this vulnerable population. Clinicians must play a larger role in advising patients to follow evidence-based nutrition recommendations. Effective strategies to integrate nutrition into oncology care need to be identified, evaluated, and implemented to close this gap. It is also important to recognize that cancer patients and survivors may encounter barriers that may prevent them from adhering to nutrition recommendations. In addition, some patients may prefer dietary strategies that are consistent with their cultural and ethnic backgrounds. At the end of the day, nutrition recommendations need to be patient-centered to achieve success.FINANCIAL DISCLOSURE: Dr. Zhang has no significant financial interest in or other relationship with the manufacturer of any product or provider of any service mentioned in this article.
Only two studies have investigated the role of dietary acid load and cancer. One prospective cohort study examined the association between bladder cancer risk and urine pH in 27,096 male smokers enrolled in the Alpha-Tocopherol, Beta-Carotene Cancer Prevention (ATBC) Study. The relative risk (RR) for developing bladder cancer was not significantly associated with urine pH (RR, 1.15; 95% CI, 0.86–1.55) when comparing the highest to the lowest urine pH. However, in men who had smoked for longer than 45 years, there was suggested increased risk with lower urine pH levels (RR, 1.72; 95% CI, 0.96–3.10; P = .08).[20] Another small open-label study examined use of an alkaline diet in 11 advanced or recurrent non–small-cell lung cancer patients who were receiving an EGFR tyrosine kinase inhibitor. While patients had longer than expected median progression-free survival (19.5 months; range, 3.1–33.8 months) and overall survival (28.5 months; range, 15.4–46.6 months), there was no control group; thus, findings are difficult to interpret.[21] In sum, the logic behind the alkaline diet is faulty, and evidence is lacking. Despite this, the alkaline diet is highly congruent with dietary recommendations for cancer patients and survivors. As such, it may be appropriate for cancer patients, but for reasons different than those given by proponents (See Figure).
Paleolithic Diet
The Paleolithic diet attempts to replicate the dietary pattern of Stone-Age humans, featuring foods readily available to hunter-gatherers, including fruits, vegetables, nuts, meat, and eggs, while excluding grains, legumes, dairy products, and all processed foods (see Table).[22] The diet’s rationale is based on the idea-known as the “evolutionary discordance hypothesis”-that humans evolved for millennia with a relatively consistent diet, and that chronic diseases such as cancer arise from the consumption of foods available only after the agricultural revolution, which humans are not genetically equipped to digest.[23] Proponents of the diet assume that human genes have not changed significantly since the Paleolithic period ending about 10,000 years ago, that there is an understanding of prehistoric diets, and that the foods available historically are equivalent to modern foods. Each of these assumptions is, however, contradicted by anthropological evidence that there is no single Paleolithic diet; that grains have been processed and consumed in Europe for more than 40,000 years; that humans have recently evolved to eat foods prominent in their environment, as evidenced by the development of lactase persistence in Europe and Africa; and that foods available today have been considerably altered by human agricultural practices and are thus substantially different than those foods available historically.[24-27] Moreover, cancer is a disease that tends to occur late in life, after one has passed prime reproductive age, and thus does not exert selection pressure in a population for a lower incidence of cancer.
Evidence for the Paleolithic diet in cancer prevention or treatment is limited to two case-controlled studies. In one study, the highest adherence to a Paleolithic dietary pattern compared with the lowest adherence was associated with reduced all-cause mortality (hazard ratio [HR], 0.72; 95% CI, 0.55–0.95; P = .03).[28] In a similar study, the odds of colorectal adenoma were lower among those in the highest quintile of adherence to Paleolithic dietary pattern when compared with disease-free controls (adjusted odds ratio, 0.71; 95% CI, 0.50–1.02; P = .02).[29] The Paleolithic diet has an emphasis on fruit, vegetables, nuts, and seeds, while restricting refined carbohydrates, processed meats, and alcohol. However, the diet opposes AICR dietary guidelines by being high in saturated fat and low in legumes and cereal grains, a combination associated with worsened colorectal cancer survival.[30] In conclusion, the Paleolithic diet shares characteristics with other healthy diets, but strict adherence may eliminate food groups proven to be beneficial for cancer prevention and general health (See Figure).
Ketogenic Diet
Ketogenic diets are high-fat, low-carbohydrate, adequate-protein diets with a macronutrient ratio of 3–4:1 of fat to protein and non-fiber carbohydrates. Sixty-five percent or more of calories come from fat, while carbohydrate intake is restricted to 20 to 60 grams per day (see Table).[31] This macronutrient composition forces the body to metabolize lipids rather than carbohydrates or proteins, and shifts the body’s primary energy substrate from glucose to ketones. Per the Warburg effect-the phenomenon that cancer cells rely on glycolysis to fuel growth even in the presence of oxygen-proponents hypothesize that cancer cell growth will be hampered by a shift to ketone metabolism.[32] Evidence suggests that some cancer cells appear less able to metabolize ketones compared with healthy cells, while other experiments show that some tumor cells are able to use ketones for energy.[33]
More recently, however, preclinical research suggests that the potential mechanism of ketosis on cancer cells does not rely solely on the Warburg effect. The spectrum of altered growth, metabolism, and signaling metabolites incurred by ketosis may result in a cancer cell–specific induction of oxidative stress, thereby potentiating the effect of chemotherapy and radiation.[34,35] Additionally, ketogenic diets may have a protein-sparing effect that preserves lean body mass in the setting of cancer cachexia.[36] In animal models, ketogenic diets decrease the initiation, progression, and metastasis of cancer.[37]
Evidence in human clinical trials is limited to cases and small open-label studies, typically as salvage therapies, which confirm the feasibility and safety of ketogenic diets. These studies suggest that ketogenic diets are safe, and do not negatively impact quality of life. They are, however, difficult to adhere to, and many patients do not reach desired levels of ketones in the urine.[35,38-41] The bottom line is that ketogenic diets may have utility in certain individuals, especially in combination with other conventional therapies, but there is currently no reliable way to predict which patients might respond. They are exceedingly difficult to implement without professional dietary counseling. Moreover, poorly implemented ketogenic diets incur risk for micronutrient deficiency; are very high in saturated fat; are typically low in fiber; may include processed foods; and may exclude entire food groups, such as fruits, legumes, and many vegetables, which have been shown to be beneficial for cancer prevention and mortality (See Figure).
Vegan Diet
A vegan diet entails abstinence from the consumption of animal products, such as meat, fish, eggs, dairy, and honey (see Table).[42] This is in contrast to plant-based diets, which consist mostly of fruits, vegetables, legumes, nuts/seeds, and whole grains, as well as small amounts of eggs, dairy, fish, fowl, and red meat. Vegan diets are often adopted for ethical or philosophical reasons focused on animal welfare or environmental conservation. Eating a vegan diet is thought to increase intake of so-called “cancer-fighting” foods, such as berries, greens, whole grains, nuts, and seeds, while eliminating foods such as dairy products and red and processed meats that may increase cancer risk.[43,44] A meta-analysis of 24 cross-sectional studies and 4 prospective cohort studies found that vegan diets were associated with a 15% risk reduction in total cancer incidence (RR, 0.85; 95% CI, 0.75–0.95), although no difference was observed for mortality.[45] Also, several small randomized clinical trials in men with low-risk prostate cancer showed benefits of a low-fat (~10% total fat) vegan diet in decreasing prostate-specific antigen levels,[46] lengthening telomeres,[47] positively impacting prostate gene expression,[48] and improving quality of life.[49] The vegan diet, however, was delivered along with exercise, stress reduction, and social support, making it hard to determine how much the diet itself contributed to results.
It is also unclear whether avoiding all animal products is necessary for obtaining the positive health benefits of a vegan diet. Vegetarian diets were associated with an 8% reduced risk in total cancer incidence.[45] Also, when looking at colorectal cancer incidence in a prospective cohort study (The Adventist Health Study 2) of 96,354 men and women, researchers found that those who ate a vegetable-based diet with the addition of seafood had the lowest risk (43%; HR, 0.57; 95% CI, 0.40–0.82), while vegans and vegetarians had similar risk reductions (19% and 18%, respectively) when compared with non-vegetarians.[50] In addition, the evidence for dairy is contradictory: high-fat dairy (not no- or low-fat) is associated with increased cancer mortality and risk of recurrence in prostate cancer and non-Hodgkin lymphoma, while dairy may be protective against colorectal cancer.[51-55] Vegan diets can be low in calcium and vitamin B12 compared with omnivorous diets, although this can be remedied by appropriate dietary advice (see Table).[56] The bottom line is that vegan diets meet many of the ACS and AICR dietary guidelines and can be fine-tuned for greater concordance (See Figure).
Macrobiotic Diet
Macrobiotics encompass a philosophy, a cultural movement, and an eating pattern that is based in large part on Eastern philosophical principles of yin and yang.[57] The macrobiotic diet is predominantly vegetarian and emphasizes unprocessed, organic foods. The diet, by weight, is 40% to 60% whole cereal grains, 20% to 30% vegetables, and 5% to 10% legumes. Fruit, white fish, seeds, and nuts are also occasionally consumed (see Table).[58] Many individuals choose macrobiotic diets for philosophical rather than health reasons alone; nevertheless, for justification, proponents point to the health benefits of a diet high in fiber, legumes, and vegetables, while also devoid of red and processed meat.[59]
There are no research studies on the macrobiotic diet in cancer patients; however, DIANA (Diet and Androgens)-5 is an ongoing randomized clinical trial in 1,208 breast cancer survivors investigating the effect of exercise and a Mediterranean-macrobiotic diet plan on weight loss and cancer recurrence.[60] The macrobiotic diet can be high in whole soy foods such as tofu, raising concerns about hormone-sensitive cancers, particularly estrogen receptor (ER)-positive breast cancer. Though there is no clinical trial investigating the impact of soy foods on breast cancer patients after diagnosis, five cohort studies in 11,206 breast cancer patients found that frequent consumption of whole soy foods (around one to three servings per day) after breast cancer diagnosis was associated with a significant 21% reduction in the risk of breast cancer recurrence; it was also associated with a 15% reduction in breast cancer mortality in both ER-negative and ER-positive cancers.[61]
The macrobiotic diet appears to meet or exceed US dietary recommendations.[62] Moreover, in a nationally representative sample, the macrobiotic diet was found to have a lower percentage of energy from fat, higher total dietary fiber, and higher amounts of most micronutrients than the Recommended Daily Allowance (RDA), with the exceptions of vitamin D, vitamin B12, and calcium, which were lower than the RDA.[62] The bottom line is that macrobiotic diets meet most of the dietary ACS and AICR guidelines, including emphasizing a healthy weight and regular physical activity (See Figure).
Conclusion
Changes in diet consistent with evidence-based clinical guidelines can have a significant impact on improving cancer incidence and mortality.[4-8] The dietary guidelines of the ACS and AICR/WCRF are framed such that compliance can be achieved with a variety of dietary patterns, including those strategies popular with cancer patients. However, the degree to which these different popular dietary strategies adhere to the dietary guidelines vary, and it is important to emphasize that there is little evidence that any element of a given diet, outside of those in accordance with evidence-based clinical dietary guidelines, will confer survival benefits. Notably, as the overall quality and quantity of evidence on these diets is limited, scientific plausibility, mechanistic evidence, and the balancing of risks and benefits are important considerations when making clinical recommendations. Moreover, many of these popular dietary strategies are chosen as much for their philosophical, cultural, or ethical underpinnings as for any scientific evidence of benefit. As such, negative or contradictory statements about a patient’s diet can lead to defensiveness and lack of trust on the part of the patient. Instead, possible strategies to build trust and encourage evidence-based dietary changes include:
1. Ask about diet, including popular diets, and structure the encounter around the “5 As” (assess, advise, agree, assist, arrange). See the discussion of nutrition counseling in clinical practice by Kahan and Manson.[63]
2. Emphasize positive aspects of these popular diet strategies that concur with ACS and AICR dietary guidelines (see Figure).
3. Refer patients to registered dieticians as needed to help guide choices.
4. Suggest foods that align with patients’ dietary strategies to address any nutrient concerns (see Table).
5. Suggest helpful resources for recipes, meal planning, serving sizes, and general dietary information congruent with ACS and AICR dietary guidelines, such as the US Department of Agriculture’s ChooseMyPlate (https://www.choosemyplate.gov), AICR (http://www.aicr.org), and Harvard T. H. Chan School of Public Health’s Healthy Eating Plate and Healthy Eating Pyramid (https://www.hsph.harvard.edu/nutritionsource/healthy-eating-plate) websites.
6. Remind patients that there is no need to adopt a strict diet that deprives them of enjoyment at mealtime to obtain the beneficial effects of dietary changes. Instead, it is helpful to mention that the effect of any diet is cumulative and long-term; thus, eating something “unhealthy” occasionally will not have any significant impact on their health.
In summary, despite limited evidence as a means of treating or preventing cancer, popular dietary patterns may appeal to cancer patients. These patients often choose to follow a diet that, with the help of clinicians, can be consistent with dietary guidelines during cancer care and supportive of overall health.
Acknowledgement: The authors wish to thank the late Fredi Kronenberg, PhD, for her inspiration in addressing this topic.
Financial Disclosure:The authors have no significant financial interest in or other relationship with the manufacturer of any product or provider of any service mentioned in this article.
References:
1. Dixon S. Nutrition in complementary and alternative medicine. Semin Oncol Nurs. 2012;28:75-84.
2. Rock CL, Doyle C, Demark-Wahnefried W, et al. Nutrition and physical activity guidelines for cancer survivors. CA Cancer J Clin. 2012;62:243-74.
3. World Cancer Research Fund/American Institute of Cancer Research. Diet, Nutrition, Physical Activity and Cancer: A Global Perspective. Continuous Update Project Expert Report 2018: American Institute of Cancer Research; 2018 May 24th 2018.
4. Balter K, Moller E, Fondell E. The effect of dietary guidelines on cancer risk and mortality. Curr Opin Oncol. 2012;24:90-102.
5. Thomson CA, McCullough ML, Wertheim BC, et al. Nutrition and physical activity cancer prevention guidelines, cancer risk, and mortality in the women’s health initiative. Cancer Prev Res (Phila). 2014;7:42-53.
6. Kabat GC, Matthews CE, Kamensky V, et al. Adherence to cancer prevention guidelines and cancer incidence, cancer mortality, and total mortality: a prospective cohort study. Am J Clin Nutr. 2015;101:558-69.
7. Jankovic N, Geelen A, Winkels RM, et al. Adherence to the WCRF/AICR Dietary Recommendations for cancer prevention and risk of cancer in elderly from Europe and the United States: A meta-analysis within the CHANCES Project. Cancer Epidemiol Biomarkers Prev. 2017;26:136-44.
8. Vergnaud AC, Romaguera D, Peeters PH, et al. Adherence to the World Cancer Research Fund/American Institute for Cancer Research guidelines and risk of death in Europe: results from the European Prospective Investigation into Nutrition and Cancer cohort study1,4. Am J Clin Nutr. 2013;97:1107-20.
9. Bishop FL, Rea A, Lewith H, et al. Complementary medicine use by men with prostate cancer: a systematic review of prevalence studies. Prostate Cancer Prostatic Dis. 2011;14:1-13.
10. Bishop FL, Prescott P, Chan YK, et al. Prevalence of complementary medicine use in pediatric cancer: a systematic review. Pediatrics. 2010;125:768-76.
11. Sewitch MJ, Rajput Y. A literature review of complementary and alternative medicine use by colorectal cancer patients. Complement Ther Clin Pract. 2010;16:52-6.
12. Saghatchian M, Bihan C, Chenailler C, et al. Exploring frontiers: use of complementary and alternative medicine among patients with early-stage breast cancer. Breast. 2014;23:279-85.
13. Fouladbakhsh JM, Stommel M. Gender, symptom experience, and use of complementary and alternative medicine practices among cancer survivors in the U.S. cancer population. Oncol Nurs Forum. 2010;37:E7-e15.
14. Mueller CM, Mai PL, Bucher J, et al. Complementary and alternative medicine use among women at increased genetic risk of breast and ovarian cancer. BMC Complement Altern Med. 2008;8:17.
15. Nestle M, Petrucci K. Big Issues in Health Care (A Special Report) - Is a Paleo Diet Healthy? Wall Street Journal, Eastern Edition 2015 23 Mar 2015.
16. Vasey C. The Acid-alkaline Diet for Optimum Health: Restore Your Health by Creating PH Balance in Your Diet. Inner Traditions/Bear & Co; 2006.
17. Jackson G. Alkaline foods for the alkaline diet: fell the pH miracle of the healthy pH diet. Createspace Independent Publishing Platform; 2014.
18. Sherman HC, Gettler AO. The balance of acid-forming and base-forming elements in foods, and its relation to ammonia metabolism. Journal of Biological Chemistry. 1912;11:323-38.
19. Buclin T, Cosma M, Appenzeller M, et al. Diet acids and alkalis influence calcium retention in bone. Osteoporos Int. 2001;12:493-9.
20. Wright ME, Michaud DS, Pietinen P, et al. Estimated urine pH and bladder cancer risk in a cohort of male smokers (Finland). Cancer Causes Control. 2005;16:1117-23.
21. Hamaguchi R, Okamoto T, Sato M, et al. Effects of an alkaline diet on EGFR-TKI therapy in EGFR mutation-positive NSCLC. Anticancer Res. 2017;37:5141-5.
22. Staffan L. Paleolithic diets as a model for prevention and treatment of western disease. American Journal of Human Biology. 2012;24:110-5.
23. Melvin K, Boyd ES. Paleolithic nutrition. Nutrition in Clinical Practice. 2010;25:594-602.
24. Gowlett JAJ. What actually was the stone age diet? Journal of Nutritional & Environmental Medicine. 2003;13:143-7.
25. Henry AG, Brooks AS, Piperno DR. Microfossils in calculus demonstrate consumption of plants and cooked foods in Neanderthal diets (Shanidar III, Iraq; Spy I and II, Belgium). Proceedings of the National Academy of Sciences. 2011;108:486-91.
26. Itan Y, Powell A, Beaumont MA, et al. The origins of lactase persistence in Europe. PLOS Computational Biology. 2009;5:e1000491.
27. Davis DR, Epp MD, Riordan HD. Changes in USDA food composition data for 43 garden crops, 1950 to 1999. J Am Coll Nutr. 2004;23:669-82.
28. Whalen KA, Judd S, McCullough ML, et al. Paleolithic and Mediterranean diet pattern scores are inversely associated with all-cause and cause-specific mortality in adults. J Nutr. 2017;147:612-20.
29. Whalen KA, McCullough M, Flanders WD, et al. Paleolithic and Mediterranean diet pattern scores and risk of incident, sporadic colorectal adenomas. Am J Epidemiol. 2014;180:1088-97.
30. Aune D, Chan DSM, Lau R, et al. Dietary fibre, whole grains, and risk of colorectal cancer: systematic review and dose-response meta-analysis of prospective studies. BMJ. 2011;343:
31. Kossoff EH, ZupecâKania BA, Amark PE, et al. Optimal clinical management of children receiving the ketogenic diet: recommendations of the International Ketogenic Diet Study Group. Epilepsia. 2009;50:304-17.
32. Hanahan D, Weinberg Robert A. Hallmarks of cancer: The next generation. Cell. 2011;144:646-74.
33.Schroeder U, Himpe B, Pries R, et al. Decline of lactate in tumor tissue after ketogenic diet: In vivo microdialysis study in patients with head and neck cancer. Nutrition and Cancer. 2013;65:843-9.
34. Allen BG, Bhatia SK, Anderson CM, et al. Ketogenic diets as an adjuvant cancer therapy: History and potential mechanism. Redox Biol. 2014;2:963-70.
35. Zahra A, Fath MA, Opat E, et al. Consuming a ketogenic diet while receiving radiation and chemotherapy for locally advanced lung and pancreatic cancer: The University of Iowa experience of two phase I clinical trials. Radiation Research. 2017;187:743-54.
36. Shukla SK, Gebregiworgis T, Purohit V, et al. Metabolic reprogramming induced by ketone bodies diminishes pancreatic cancer cachexia. Cancer & Metabolism. 2014;2:18.
37. Lv M, Zhu X, Wang H, et al. Roles of caloric restriction, ketogenic diet and intermittent fasting during initiation, progression and metastasis of cancer in animal models: a systematic review and meta-analysis. PLoS One. 2014;9:e115147.
37. Schroeder U, Himpe B, Pries R, et al. Decline of lactate in tumor tissue after ketogenic diet: In vivo microdialysis study in patients with head and neck cancer. Nutrition and Cancer. 2013;65:843-9.
38. Klement RJ. Beneficial effects of ketogenic diets for cancer patients: a realist review with focus on evidence and confirmation. Medical Oncology. 2017;34:132.
39. Schmidt M, Pfetzer N, Schwab M, et al. Effects of a ketogenic diet on the quality of life in 16 patients with advanced cancer: A pilot trial. Nutr Metab (Lond). 2011;8:54.
40. Rieger J, BÃHr O, Maurer GD, et al. ERGO: A pilot study of ketogenic diet in recurrent glioblastoma. International Journal of Oncology. 2014;44:1843-52.
41. Tan-Shalaby JL, Carrick J, Edinger K, et al. Modified Atkins diet in advanced malignancies - final results of a safety and feasibility trial within the Veterans Affairs Pittsburgh Healthcare System. Nutrition & Metabolism. 2016;13:52.
42. Francione GL. Animal welfare, happy meat, and veganism as the moral baseline. The philosophy of food. 2012;169-89.
43. Bouvard V, Loomis D, Guyton KZ, et al. Carcinogenicity of consumption of red and processed meat. Lancet Oncol. 2015;16:1599-600.
44. Chan JM, Stampfer MJ, Ma J, et al. Dairy products, calcium, and prostate cancer risk in the Physicians’ Health Study. Am J Clin Nutr. 2001;74:549-54.
45. Dinu M, Abbate R, Gensini GF, et al. Vegetarian, vegan diets and multiple health outcomes: A systematic review with meta-analysis of observational studies. Crit Rev Food Sci Nutr. 2017;57:3640-9.
46. Ornish D, Weidner G, Fair WR, et al. Intensive lifestyle changes may affect the progression of prostate cancer. J Urol. 2005;174:1065-9; discussion 9-70.
47. Ornish D, Lin J, Chan JM, et al. Effect of comprehensive lifestyle changes on telomerase activity and telomere length in men with biopsy-proven low-risk prostate cancer: 5-year follow-up of a descriptive pilot study. Lancet Oncol. 2013;14:1112-20.
48. Ornish D, Magbanua MJ, Weidner G, et al. Changes in prostate gene expression in men undergoing an intensive nutrition and lifestyle intervention. Proc Natl Acad Sci U S A. 2008;105:8369-74.
49. Kronenwetter C, Weidner G, Pettengill E, et al. A qualitative analysis of interviews of men with early stage prostate cancer: the Prostate Cancer Lifestyle Trial. Cancer Nurs. 2005;28:99-107.
50. Orlich MJ, Singh PN, Sabate J, et al. Vegetarian dietary patterns and the risk of colorectal cancers. JAMA Intern Med. 2015;175:767-76.
51. Vieira AR, Abar L, Chan DSM, et al. Foods and beverages and colorectal cancer risk: a systematic review and meta-analysis of cohort studies, an update of the evidence of the WCRF-AICR Continuous Update Project. Ann Oncol. 2017;28:1788-802.
52. Aune D, Lau R, Chan DS, et al. Dairy products and colorectal cancer risk: a systematic review and meta-analysis of cohort studies. Ann Oncol. 2012;23:37-45.
53. Lu W, Chen H, Niu Y, et al. Dairy products intake and cancer mortality risk: a meta-analysis of 11 population-based cohort studies. Nutr J. 2016;15:91.
54. Tat D, Kenfield SA, Cowan JE, et al. Milk and other dairy foods in relation to prostate cancer recurrence: Data from the cancer of the prostate strategic urologic research endeavor (CaPSURE). Prostate. 2018;78:32-9.
55. Wang J, Li X, Zhang D. Dairy Product Consumption and Risk of Non-Hodgkin Lymphoma: A Meta-Analysis. Nutrients. 2016;8:120.
56. Melina V, Craig W, Levin S. Position of the Academy of Nutrition and Dietetics: Vegetarian Diets. J Acad Nutr Diet. 2016;116:1970-80.
57. Kushi M, Jack A. The book of macrobiotics: the universal way of health, happiness, and peace. Japan Publications; 1986.
58. Kushi M, Jack A. The Cancer Prevention Diet: Michio Kushi’s Macrobiotic Blueprint for the Prevention and Relief of Disease. 1993; Martin’s Press: New York, NY.
59. Kushi LH, Cunningham JE, Hebert JR, et al. The macrobiotic diet in cancer. J Nutr. 2001;131:3056s-64s.
60. Villarini A, Pasanisi P, Traina A, et al. Lifestyle and breast cancer recurrences: the DIANA-5 trial. Tumori. 2012;98:1-18.
61. Chi F, Wu R, Zeng YC, et al. Post-diagnosis soy food intake and breast cancer survival: a meta-analysis of cohort studies. Asian Pac J Cancer Prev. 2013;14:2407-12.
62. Harmon BE, Carter M, Hurley TG, et al. Nutrient Composition and Anti-inflammatory Potential of a Prescribed Macrobiotic Diet. Nutr Cancer. 2015;67:933-40.
63. Kahan S, Manson JE. Nutrition Counseling in Clinical Practice: How Clinicians Can Do Better. JAMA. 2017;318:1101-2.
64. Manousou S, Stål M, Larsson C, et al. A Paleolithic-type diet results in iodine deficiency: a 2-year randomized trial in postmenopausal obese women. Eur J Clin Nutr. 2018;72:124.
65. Hoffman R. Can the paleolithic diet meet the nutritional needs of older people? Maturitas. 2017;95:63-4.
66. Le LT, Sabate J. Beyond meatless, the health effects of vegan diets: findings from the Adventist cohorts. Nutrients. 2014;6:2131-47.
67. Schwalfenberg GK. The alkaline diet: is there evidence that an alkaline pH diet benefits health? J Environ Public Health. 2012;2012:727630.
Related Videos
Related Content







