Multiple Myeloma
Latest News


April 12th 2024
Minimal residual disease can now be considered an end point in trials leading to accelerated approvals by the FDA for multiple myeloma.


















Equalizing Inequities™ in Multiple Myeloma Care: Shining a Light on Current Barriers and Opportunities for Improved Outcomes
View More

Patient, Provider, and Caregiver Connection: Addressing Pediatric and AYA Patient Concerns While Managing Hodgkin Lymphoma
View More

Patient, Provider, and Caregiver Connection™: Individualizing Care for Patients with Schizophrenia—Understanding Patient Challenges and the Role of Innovative Treatment
View More
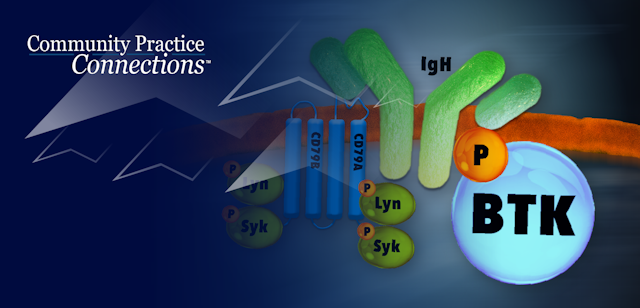
B-Cell Tumor Board: Rendering Real World Personalized Treatment Plans in CLL/SLL and MCL Through the Lens of Emerging BTKi Evidence
View More
Applying New Evidence in Multiple Myeloma Care from Frontline to R/R Disease
View More

Community Oncology Connections™: Overcoming Barriers to Testing, Trial Access, and Equitable Care in Cancer
View More
Translating New Evidence into Treatment Algorithms from Frontline to R/R Multiple Myeloma: How the Experts Think & Treat
View More

Medical Crossfire: How Has Iron Supplementation Altered Treatment Planning for Patients with Cancer-Related Anemia?
View More

Medical Crossfire®: The Experts Bridge Recent Data in Chronic Lymphocytic Leukemia With Real-World Sequencing Questions
View More
Improving Outcomes in Autoimmune Hemolytic Anemias at the Intersection Between Hematology and Oncology Care
View More

Community Practice Connections™: 5th Annual Precision Medicine Symposium – An Illustrated Tumor Board
View More
More News













Guiding Through Challenges: Insights for Caregivers of R/R MM Patients
February 1st 2024Ursula Linne-Mclaren briefly discusses valuable guidance for patients and caregivers, particularly those considering bispecific therapies, providing a supportive perspective on the journey through R/R MM treatment.

Patient-Centric Care in R/R MM
February 1st 2024Nurse Linne-Mclaren provides her insights into the proactive measures, monitoring strategies, and experiences related to talquetamab-associated adverse events, along with a broader perspective on prophylactic measures for managing potential adverse events in bispecific therapies.



Ide-cel or Standard Regimens in Relapsed and Refractory Multiple Myeloma
Compare outcomes between ide-cel chimeric antigen receptor T-cell (CAR-T) therapy and standard treatment regimens such as pomalidomide and daratumumab combinations in patients with heavily pretreated relapsed and refractory multiple myeloma.

Collaborative Care and Access Challenges in Managing R/R MM with GPRC5D Bispecific
January 25th 2024Oncology Clinical Pharmacist Specialist Amir Ali delves into potential challenges related to access and the use of this therapy, providing a comprehensive perspective on the complexities of incorporating GPRC5-targeting bispecifics into R/R MM patient management.

Present real-world data on the efficacy and safety of the ixazomib-lenalidomide-dexamethasone combination in patients with relapsed/refractory multiple myeloma outside of clinical trials.

Outcomes After Biochemical or Clinical Progression in Patients With Multiple Myeloma
Examine outcomes such as overall survival, progression-free survival, and response rates in multiple myeloma patients who have experienced biochemical or clinical progression after prior lines of therapy.

Navigating High-Risk Disease in Multiple Myeloma: Treatment Strategies and the Role of ASCT
January 19th 2024Experts dive into the complexities of defining and treating high-risk Multiple Myeloma (MM) and discuss the role of ASCT in newly diagnosed MM and weigh the considerations for recommending transplants, including insights on the selection criteria for tandem transplantations.

