

































































Results of a combined analysis of SWENOTECA studies showed that surveillance remains a good option for patients with stage I seminoma testicular cancer.
Results of a combined analysis of SWENOTECA studies showed that surveillance remains a good option for patients with stage I seminoma testicular cancer.
The addition of gemcitabine to a cisplatin- and ifosfamide-containing drug regimen resulted in a complete response rate of greater than 50% in patients with relapsed metastatic germ cell tumors, results of a phase II study indicated.

Cisplatin-based chemotherapy has transformed the prognosis of testicular germ cell cancer (GCT). It has converted the chief mortal malignancy in younger men into a model for the curability of cancer.

Germ cell tumors (GCT) are an exemplar of the successful use of chemotherapy and of the successful interplay of phase II and phase III trials. The biggest contributor to cure in metastatic GCT is cisplatin-based chemotherapy, unchallenged after more than 30 years.

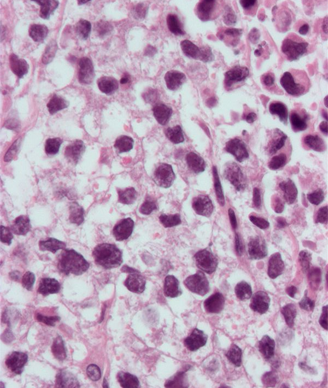
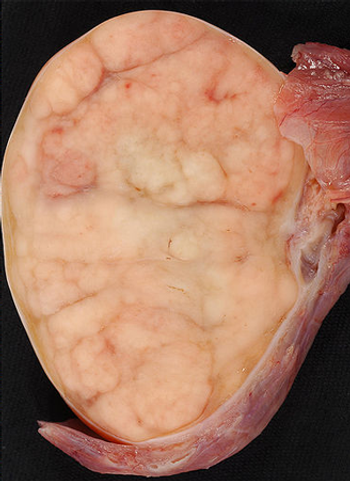
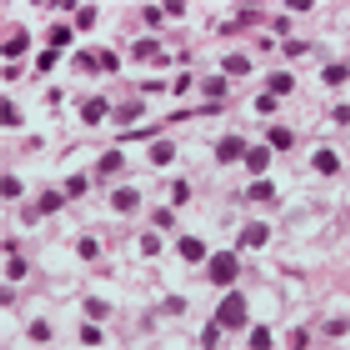
A 22-year-old man presented to the emergency department with a 5-cm painful testicular mass that had increased in size over the previous month. Tumor markers were drawn and an inguinal orchiectomy was performed.
At the 2013 ASCO meeting, investigators of a large Danish study have concluded that surveillance alone following surgery for stage I seminoma is sufficient, sparing patients in this setting from the unnecessary expense and associated toxicities of chemotherapy and radiation treatment.
Dr. Bruce Roth, Siteman Cancer Center, spoke at the 2013 ASCO meeting about topics in seminoma. Here he discusses recurrence, relapse, and seminomatous vs nonseminomatous testicular cancer.
Dr. Bruce Roth, Professor of Oncology in the Division of Medicine at Siteman Cancer Center, Washington University at St. Louis, spoke at the 2013 ASCO meeting about topics in seminoma. Here he discusses the epidemiology of seminoma.
Dr. Bruce Roth discusses the large Danish study reported at ASCO (abstract 4502) that showed surveillance alone is sufficient after orchiectomy for stage I seminoma.
Dr. Bruce Roth discusses the large Danish study reported at ASCO (abstract 4502) that showed surveillance alone is sufficient after orchiectomy for stage I seminoma, focusing on its impact on post-surgery radiation therapy in this setting.
Surveillance of patients with stage I seminoma following orchiectomy can spare a majority of patients from adjuvant chemotherapy with a low risk of relapse, according to results presented at the 2013 ASCO meeting.
Two genome-wide studies have identified a total of 12 new genetic loci associated with a higher risk of testicular cancer. The risk-associated genetic variations could help clinicians single out higher-risk men for screening and early detection.

Researchers have linked recreational marijuana use to an increased risk of developing germ-cell tumors, a type of testicular cancer that often has a poor prognosis.
Two experts discuss newly available and upcoming treatment options, such as abiraterone and MDV3100, for patients with castration-resistant prostate cancer.
There is a lack of scientific evidence about the risk of testicular cancer associated with testicular lesions, but the conventional treatment approach has been immediate surgical removal because of the possibility of malignancy. A more conservative approach has served one Canadian institution well when it comes to active surveillance of small, incidentally discovered testicular masses.
Hammerich et al. report a case of synchronous bilateral germ cell tumors (GCT) of different histologies occurring in a patient with a history of cryptorchidism. There are several interesting aspects of this case and the authors’ management and discussion that warrant commentary.
A 36-year-old male with a history of cryptorchidism of the right side, treated with orchidopexy at the age of 4, presented with bilateral testicular swelling. Investigations included laboratory workup, ultrasound of both testes, as well as CT-scan of the chest, abdomen, and pelvis. Initial treatment was bilateral orchiectomy.
Osteopenia and osteoporosis are increasingly common in cancer patients, owing to the aging of the population and to new forms of cancer treatment. Androgen and estrogen deprivation, as well as some forms of cytotoxic chemotherapy, may lead to osteopenia and osteoporosis. Patients at risk for osteoporosis include those treated with aromatase inhibitors and with androgen deprivation for more than 1 year. In addition, all patients 65 years of age and older are at risk of osteoporosis when treated with cytotoxic agents, and so should be screened for bone loss. Several treatments have been effective in the prevention and management of osteoporosis. In patients at risk for this complication, it is recommended to obtain a bone density evaluation and to start appropriate treatment. This may include calcium and vitamin D supplementation for mild forms of osteopenia, and bisphosphonate therapy or denosumab (Prolia) for more advanced osteopenia and osteoporosis.

Listen to internationally regarded oncologist and clinical investigator, Robert J. Motzer, MD, attending physician at Memorial Sloan-Kettering Cancer Center, discuss the past, present, and future trends in renal cell carcinoma.
Hematopoietic malignancies account for 6% to 8% of new cancers diagnosed annually. In the year 2009, an estimated 44,790 new cases of leukemia were diagnosed, and 21,870 deaths were attributable to leukemias of all types. The total age-adjusted incidence of leukemia, including both acute and chronic forms, is 9.6 per 100,000 population; the incidence of acute lymphoblastic leukemia (ALL) is 1.5 per 100,000 and of acute myelogenous leukemia (AML) is 2.7 per 100,000 population.
In my practice as an oncologist specializing in gastrointestinal tract cancers, a recent week was fairly typical. I saw 50 patients, ranging in age from 32 to 87, equally divided between men and women. Though a couple of them have inherited a gene that may have caused their GI cancers, I have no explanation for why most developed their disease. It is as if they were simply struck by lightning.
There is a complex array of tests for imaging the abdomen, but there are really only three things that oncologists need to tell radiologists in order to get the most from these imaging studies, according to Fergus V. Coakley, MD, chief of abdominal imaging at the University of California, San Francisco. “We need you to tell us the working diagnosis; what treatment the patient has had; and, the most critical, what is the question you want answered by this test? That’s the most important one,” Dr. Coakley said during a presentation at ASCO 2009 in Orlando.
We have presented the first case of a patient with metastatic ATGCT with peritoneal carcinomatosis, who responded to treatment with a VEGFR tyrosine kinase inhibitor. Because of the relative paucity of such cases in the literature, no clear treatment strategy exists. For patients with metastatic ATGCT, enrollment in clinical trials testing novel therapies, including angiogenesis inhibitors, is a reasonable option.
Granulosa cell tumors of the testis are very rare neoplasms. While most appear to have a benign course, they occasionally metastasize.
Over the past 3 decades, the incidence rate of testicular seminoma has continually risen, and the majority of cases have been clinical stage I.[1] Nevertheless, the overall survival for all testicular cancers has improved significantly (P < .05) over the same period, from 83% to 96%.[2]