Liso-Cel Yields Long-Lasting Responses in Relapsed/Refractory Large B-Cell Lymphoma
Patients with relapsed/refractory large B-cell lymphomas experienced durable responses to treatment with lisocabtagene maraleucel.
Treatment with lisocabtagene maraleucel (liso-cel; Breyanzi) resulted in long-lasting responses in patients with relapsed/refractory large B-cell lymphomas (LBCL), according to the 2-year follow-up analysis of the phase 1 TRANSCEND NHL 001 trial (NCT02631044) that was presented at the 2022 Tandem Meeting.1
Treatment with liso-cel resulted in an overall response rate (ORR) of 73% (95% CI, 66.9%-78.1%), including a complete response (CR) rate of 53% (95% CI, 46.6%-59.2%) after a median follow-up of 23.0 months. The median duration of response (DOR) by Lugano 2014 criteria was 23.1 months (95% CI, 8.6–not reached [NR]) and the probability of continued response at 2 years was 49.5% (95% CI, 41.4%-57.0%).2 Additionally, the median DOR was 26.1 months (95% CI, 23.1–NR) and 23.1 months (95% CI, 5.6-NR) in those who achieved a CR and partial response (PR), respectively.
“This 2-year follow-up analysis of TRANSCEND demonstrated durable response to liso-cel in patients with high-risk aggressive relapsed/refractory LBCLs,” Jeremy Abramson, MD, director of the Jon and Jo Ann Hagler Center for Lymphoma, Massachusetts General Hospital, and an associate professor of medicine at Harvard Medical School said during the presentation. He continued “Liso-cel treatment was associated with a low incidence of severe cytokine release syndrome [CRS] and neurologic events.”
To be eligible for the study, patients needed to be 18 years or older and have received 2 or more prior lines of therapy. Those who enrolled had diffuse large B-cell lymphoma that was not otherwise specified (DLBCL NOS)—either de novo or transformed from follicular lymphoma, marginal zone lymphoma, or another disease—high-grade B-cell lymphoma (HGBCL), primary mediastinal large B-cell lymphoma (PMLBCL), or follicular lymphoma grade 3B (FL3B). Other inclusion criteria included previous hematopoietic stem cell transplant and an ECOG performance status of 0 or 2. Primary central nervous system lymphoma was also allowed.
Patients received a lymphodepleting regimen of 30 mg/m2 fludarabine and 300 mg/m2 of cyclophosphamide for 3 days followed by liso-cel 2 to 7 days later. The on-study follow up was 24 months.
The study’s primary end points were adverse effects (AE) and ORR by independent review committee (IRC). Secondary end points included CR rate by IRC, DOR, progression-free survival (PFS), overall survival (OS), and pharmacokinetic profile.
Patients who enrolled on the trial were followed for 2 years after the last liso-cel dose, and the study is ongoing as of the cutoff date of January 2021. Two hundred and sixty-eight patients had died or withdrawn 24 months or more after follow-up. Among 120 patients in the liso-cel set who completed the study, 81 agreed to be part of a long-term follow-up study assessing safety and OS up to 15 years, but no IRC response assessments were performed.
Notably, 1 patient died following an ongoing CR at 26 weeks due to sepsis. No patients relapsed after 23 months in the study.
The median patient age was 63 years and 41% of patients were aged 65 years or older. The majority of patients had DLBCL NOS (51%), and others had transformed follicular lymphoma (22%), other indolent lymphomas (7%), HGBCL (13%), PMBCL (6%), and FL3B (1%). Additionally, most patients were chemotherapy refractory (67%) and underwent treatment with a bridging therapy (59%). The overall median follow up was 19.9 months.
Additional findings from the study indicated that after a median follow-up of 23.9 months, the median PFS was 6.8 months (95% CI, 3.3-12.7) and the probability of PFS at 2 years was 40.6% (95% CI, 34.0%-47.2%). The median PFS in those who had a CR and PR was 27.3 months (95% CI, 24.0-NR) and 6.8 months (95% CI, 3.3-12.7).
After a median follow-up of 29.3 months, the median OS was 27.3 months (95% CI, 16.2-45.6), with a 2-year probability of OS rate of 50.5% (95% CI, 44.1%-56.5%).The median OS in those who had a CR or PR was 48.5 months (95% CI, 45.2-NR) and 9.0 months (95% CI, 6.0-11.4), respectively. In non-responders, the median OS was 5.4 months (95% CI, 2.9-6.5). Three deaths occurred after 45 months. Moreover, CAR T-cell persistence was detected at 48 months in the long-term follow-up study (NCT03435796) in addition to 37% of patients at 24 months in the TRANSCEND study.
In terms of safety, the most common any AEs within 90 days of infusion were neutropenia (63%), anemia (48%), and fatigue (44%), and grade 3 or higher AEs include neutropenia (60%), anemia (37%), and thrombocytopenia (27%). Any grade and grade 3 or higher infections occurred in 12% of patients, and in 41% of patients with any grade AE. From day 91 to the end of study, the most common any grade AEs were neutropenia (8%), anemia (8%), and fatigue (7%), with grade 3 or higher AEs including neutropenia (7%), anemia (6%), and thrombocytopenia (4%). Any grade and grade 3 or higher infections occurred in 5% of patients, and in 10% of patients with any grade AE.
Investigators reported several AEs of special interest. Any grade and grade 3/4 CRS were reported in 42% and 2% of patients, respectively; the median time to onset and resolution of CRS was 5 days, respectively. Any grade and grade 3/4 neurologic events were reported in 30% and 10% of patients, respectively. The median time to onset was 9 days and the median time to resolution was 11 days. Most cases of CRS and neurological events were grade 1/2, with no grade 5 events.


AEs of Special Interest From the Phase 1 TRANSCEND NHL 001 Trial
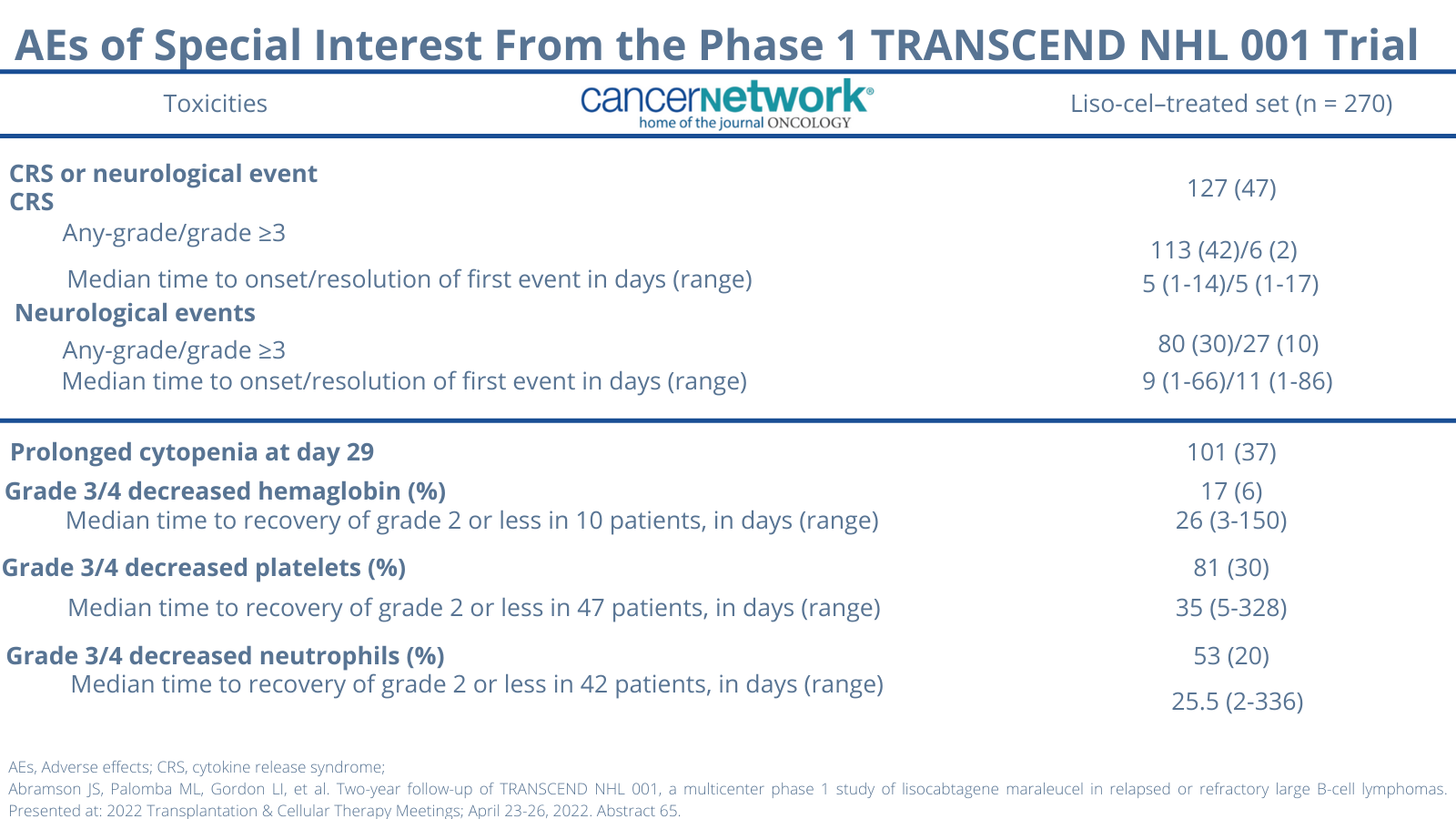
Second primary malignancies (SPM) occurred in 5 and 17 patients during the treatment emergent and post–treatment emergent periods, respectively. The types and incidence of SPMs were expected given the patient population and prior therapies and included diseases such as non-melanoma skin cancer (n = 9), solid tumors (n = 4), myelodysplastic syndrome (n = 8), acute myeloid leukemia (n = 2), and peripheral T-cell lymphoma (PTCL; n = 1). The single case of PTCL was reported on day 30 and did not appear to be in relation to treatment with liso-cel.
Of 270 patients, 9 died 30 days or less following last infusion, 24 died at over 30 days to 90 days or less, and 100 died at over 90 days. The majority of deaths were attributed to disease progression and no deaths were due to COVID-19.
References
- Abramson JS, Palomba ML, Gordon LI, et al. Two-year follow-up of TRANSCEND NHL 001, a multicenter phase 1 study of lisocabtagene maraleucel in relapsed or refractory large B-cell lymphomas. Presented at: 2022 Transplantation & Cellular Therapy Meetings; April 23-26, 2022. Abstract 65.
- Cheson BD, Fisher RI, Barrington SF, et al. Recommendations for initial evaluation, staging, and response assessment of Hodgkin and non-Hodgkin lymphoma: the Lugano classification. J Clin Oncol. 2014;32(27):3059-3068. doi:10.1200/JCO.2013.54.8800









Frontline Chemo-Free Regimen Supported in HR+/HER2+ Breast Cancer Therapy
January 1st 2024Combining anastrozole with palbociclib, trastuzumab, and pertuzumab as a frontline therapy for hormone receptor–positive, HER2-positive breast cancer may avoid some of the toxicities associated with chemotherapy, says Amy Tiersten, MD.



