
































Skin cancer is the single most common form of cancer, accounting for more than 75% of all cancer diagnoses. More than 1 million cases of squamous cell and basal cell carcinomas are diagnosed annually, with a lifetime risk of more than one in five. The vast majority of skin cancers can be cured with surgery alone. Resection is the mainstay of therapy, even for skin cancer involving regional lymph nodes or, in some cases, more distant metastatic sites.
Skin Cancer & Melanoma
Latest News
June 15th 2010
Successful Treatment of Melanoma Metastatic to the Left Atrium Using External Beam Radiation Therapy
The successful treatment of a patient with primary nasal melanoma metastatic to the lung, pulmonary vein, and left atrium using radiation therapy is described. The patient was effectively treated with a conventional external beam radiation fractionation scheme (rather than a more commonly used hypofractioned regimen) that was utilized to minimize risk of arterial embolus of the tumor or rupture of a vessel wall. A post-treatment CT demonstrated a significant decrease in the caliber of the right pulmonary vein and tumor thrombus. The patient never developed cardiac valvular dysfunction or acute life-threatening massive embolism of tumor from the atrium. Unfortunately, the patient experienced clinical decline secondary to the massive progression of intra-abdominal disease and subsequently died from multiple liver metastases and liver failure. Numerous studies and this case report demonstrate that radiation therapy can be very effective in the treatment of malignant melanoma, especially when only small volumes of disease need to be treated and adequate total doses are used. Therefore, radiation therapy appears to play an important yet underutilized role in the treatment of metastatic melanomas.
Advertisement
CME Content
Advertisement
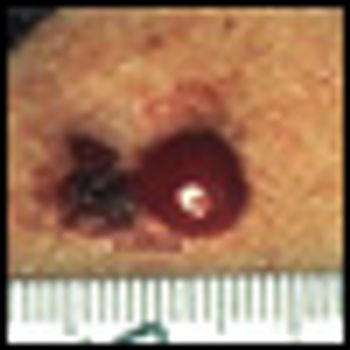
The imaging technique has the potential to measure the extent and depth of skin lesions.
CHICAGO-Radiation of the lymph nodes of high-risk melanoma patients appears to significantly reduce the risk that cancer will recur in those nodes, researchers said at ASTRO 2009. The study was deemed practice-changing, representing the first advance in the management of melanoma in nearly two decades.
The US Food and Drug Administration’s (FDA) Oncologic Drugs Advisory Committee (ODAC) recommended approval by a vote of six to four for pegylated interferon alfa-2b (PegIntron) in the adjuvant treatment of patients with stage III malignant melanoma.
Pattern analyses reveal clues to better patient management
Patients with unresectable stage III or IV melanoma taking ipilimumab and the oral steroid budesonide to reduce side effects did not have less diarrhea, according to results of a phase II trial.
Antioxidant supplements are not associated with an increased risk of melanoma, according to results from the Vitamins and Lifestyle study.
A virus discovered last year in a rare form of skin cancer has also been found in people with the second most common form of skin cancer among Americans, according to researchers at the Ohio State University Comprehensive Cancer Center–James Cancer Hospital and Solove Research Institute. Their findings were published online June 25, 2009, by the Journal of Investigative Dermatology.
Melanoma continues to be a poorly understood and frequently under-recognized cancer threat to society. The authors have provided a comprehensive overview of this malignancy from diagnosis to advanced-stage therapy.

Melanoma affects persons of all ages, causing more years of lost life than any other cancer except leukemia.[1] The American Cancer Society estimates that about 68,720 new melanomas will be diagnosed in the US in 2009, with more than 8,650 deaths, and an estimated lifetime risk of 1 in 50 for whites, 1 in 200 for Hispanics, and 1 in 1,000 for blacks.[2]
Synta and GlaxoSmithKline will end their agreement to develop and market elesclomol for the treatment of metastatic melanoma after lackluster results from the SYMMETRY trial.
Preliminary findings from a phase III, multicenter trial show that adding a novel cancer vaccine-called gp100:209-217(210M) peptide-to standard therapy doubles response rates and extends progression-free survival in patients with metastatic melanoma, without causing significant side effects (abstract CRA9011).
PHOENIX, Ariz.-In patients with intermediate thickness localized melanoma, wide excision surgery is usually curative, but metastasis to regional lymph nodes can occur. Some clinicians advocate immediate elective lymphadenectomy in these patients who have positive sentinel node biopsies as a way to improve tumor staging and survival.
Annually, about 8,000 patients are found to have metastatic melanoma presenting as recurrence of an earlier primary melanoma, and this number closely approximates the annual number of deaths from the disease. This statistic illustrates the lack of progress that has been made in the treatment of stage IV melanoma over the past several decades.
Reviewing treatment modalities for melanoma provides many sobering reminders that advances in our scientific understanding have not yet translated into meaningful clinical benefit. As clearly delineated by the authors, the “standard” treatment of dacarbazine chemotherapy has a poor response rate and lacks durability.
The article by Bhatia and colleagues focuses on the treatment of patients with metastatic melanoma using standard therapies, but it also includes a brief outline of recent treatment approaches using investigational agents. In addition, the authors describe prognostic factors for metastatic melanoma, highlighting the impact of the extent of tumor and the site of metastasis (eg, soft-tissue vs visceral metastases) on survival.
Metastatic melanoma continues to be a challenging disease to treat, with an estimated 8,420 related deaths in the United States in 2008.[1] The 10- year survival rate for patients with metastatic melanoma is less than 10%.[2] More than 3 decades after its initial approval by the US Food and Drug Administration (FDA) in 1975, dacarbazine continues to be the standard of care for most patients with this disease. High-dose interleukin-2 (HD IL-2 [Proleukin]), approved by the FDA in 1998 for metastatic melanoma, benefits a small subset of patients.

The recommendation to minimize sun exposure to prevent skin cancer has produced a pandemic of vitamin D deficiency. Vitamin D has generated considerable interest in the past decade, as accumulating evidence from both retrospective and prospective epidemiologic studies suggests an association between vitamin D deficiency and increased risk of autoimmune, infectious, and cardiovascular diseases, as well as cancer.
It is estimated that more than 62,000 men and women will be diagnosed with melanoma in 2008, with more than 8,400 deaths, and an estimated lifetime risk predicted to be 1 in 55.[1] Although deadly in its later stages, melanoma carries an excellent prognosis if it is diagnosed early. Fortunately, most melanoma cases (80%) are diagnosed at a localized stage; the 5-year survival rate for this group is 98.5%.
Melanoma frequently metastasizes to the small bowel. In this installment of Clinical Quandaries, we describe the case of 74-year-old man who presented with this rare but well described manifestation of malignant melanoma
Small bowel metastases from melanoma are uncommon. While the authors reference two studies that reported a large proportion of patients with small bowel metastases, the true incidence of gastrointestinal (GI) lesions in melanoma patients is much lower.

The University of Colorado Health Sciences Center holds weekly second opinion conferences focusing on cancer cases that represent most major cancer sites. Patients seen for second opinions are evaluated by an oncologist.
STOCKHOLM-Elesclomol, an investigational small-molecule oxidative stress inducer (Synta Pharmaceuticals), in combination with paclitaxel (Taxol) showed a trend toward improved survival in stage IV metastatic melanoma patients, compared with paclitaxel alone.
During this election year, approximately 1.4 million U.S. residents will be diagnosed with cancer. For U.S. presidential hopefuls Sen. Barack Obama and Sen. John McCain, cancer has hit close to home. Sen. McCain, 72, has been treated several times for squamous cell carcinoma and malignant melanoma. Sen. Obama lost his grandfather to prostate cancer and his mother to ovarian cancer.
The natural history of melanoma has changed little over the years, despite advances in testing and treatment such as cytotoxics, DNA-damaging agents, antimicrotubule drugs, and immunomodulatory therapies. Only 15% of advanced-stage patients respond to the two FDA-approved agents, interleukin-2 and dacarbazine (DTIC or DTIC-Dome).
Advertisement
Advertisement
Trending on CancerNetwork
1
Modifiable Risk Factors Suggest Potential for Improving Cancer Prevention
2
Barriers to CAR T-Cell Referral and Center Access in Multiple Myeloma
3
2026 Tandem Meetings: What’s the Latest Research in Multiple Myeloma?
4
Real World Outcomes of CAR T-Cell Therapy in Multiple Myeloma Including Older and Comorbid Patients
5