
So-called “narrow network” healthcare plans are more likely to exclude oncologists who are associated with NCI-designated or NCCN Cancer Centers, according to a new study.
So-called “narrow network” healthcare plans are more likely to exclude oncologists who are associated with NCI-designated or NCCN Cancer Centers, according to a new study.
Participating in a palliative care consultation significantly decreased healthcare use of Medicare beneficiaries with advanced cancer at the end of life.

In this interview we discuss a recent study that linked periodontal disease with an increased cancer risk, specifically melanoma and cancers of the lung, breast, esophagus, and gallbladder.
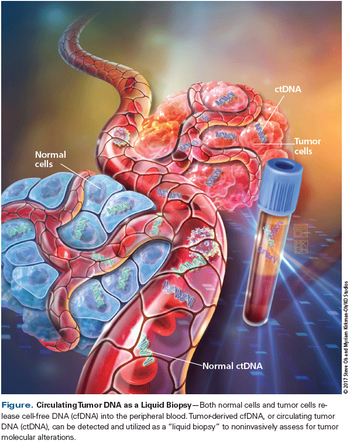
Here we review the clinical data supporting these different plasma genotyping methodologies, and present a practical approach to the interpretation of the results of these tests.

In this interview we discuss the issue of burnout in oncology, including signs and risk factors, how it might affect patient care, and strategies for prevention.

With some analyses warning of an impending oncologist shortage, are we truly approaching a point of critical need? Are practice extenders such as advanced practitioners the best solution to fill that gap or are there other options?
A Florida doctor was sentenced to serve nearly 6 years in prison for a variety of charges relating to her use of fraudulent medications to treat cancer patients.

Opioid prescriptions were significantly higher among cancer survivors compared with controls, even years after attaining survivorship.
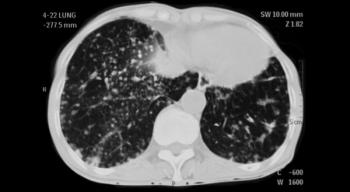
Computed tomography (CT) screening for lung cancer could lead to increased rates of smoking cessation in a high-risk population, with this “teachable moment” extending even to those with negative scan results.
Surgical management of the patient with non–small-cell lung cancer (NSCLC) is complex. When should stereotactic body radiation therapy be used? What are the advantages of video-assisted thoracic surgery? Test your knowledge in our latest quiz.
Breast cancer subtypes generally did not respond differently to radiotherapy following breast-conserving surgery, according to long-term follow-up of a randomized trial.

The US Food and Drug Administration has approved the tyrosine kinase inhibitor ibrutinib (Imbruvica) for adult patients with chronic graft vs host disease who have failed on one or more lines of prior systemic therapy.

The FDA has announced a new comprehensive plan for tobacco and nicotine regulation designed to serve as a road map to better protect American children and reduce tobacco-related disease and death.

In our latest ongoing cartoon series set in the world of oncology and cancer care, a radiologist uncovers a known risk factor.
Adherence to screening protocols at cancer centers resulted in fewer emergency department visits and hospitalizations in the 2-month period after the screening.

This video reviews the mechanisms of acquired and upfront endocrine resistance in estrogen receptor–positive breast cancer as well as research into strategies for overcoming this resistance.

This video discusses chemotherapy decision-making in early-stage breast cancer, and reviews tools such as PREDICT 2.0 and the MammaPrint 70-gene assay that can help guide treatment.

The FDA has expanded the indication for a scalp cooling device that reduces hair loss during chemotherapy.
More privately insured cancer patients seeking to participate in clinical trials received approval since the passage of the Affordable Care Act, according to a new study.

This video examines how planned radiation will impact management of the axilla in breast cancer patients undergoing mastectomy.
The understanding of the relationship between genetic variation and an individual patient’s response to radiation therapy has gained significant ground over the past several years. Genetic markers have been identified that could ultimately serve as the foundation for predictive models in clinical practice, and that hold the potential to revolutionize the delivery of precision medicine in oncology.

In this interview we discuss the goals of the Community Oncology Alliance, highlights from their annual meeting, and the challenge of transitioning cancer care to the hospital setting.
As specific candidate genes become more well established and gene expression assays gain sophistication, the value in clinical outcomes prediction and treatment selection is expected to transform the practice of radiation oncology.
A 70-gene expression score can identify women with indolent breast cancer at “ultralow” risk, according to a new study. Women with such a score have extremely low risk of disease-specific mortality over 20 years without systemic therapy.
Proton-beam therapy was found to be safe for patients with limited-stage small-cell lung cancer in the first prospective registry study of the therapy, with only a small number of high-grade toxicities.
A combination of netupitant and palonosetron was non-inferior to aprepitant plus granisetron in preventing chemotherapy-induced nausea and vomiting.

This video reviews new studies examining the genetic drivers of three rare genitourinary cancers: von Hippel-Lindau disease, advanced papillary renal cell carcinoma, and penile cancer.

Dear Patient-Although the circumstances were stressful, it was indeed a pleasure meeting you and your family today. There are words I wanted to say to you today but didn’t, for fear of distracting you from the immediate plan and also, I must admit, out of a certain degree of evasiveness.

This video reviews the management approach for prostate cancer in older patients, including when screening is appropriate and how geriatric assessments can guide treatment decisions.
What is the effect of statin use on overall survival in elderly patients with platinum-resistant ovarian cancer? Do you know the cumulative ovarian cancer risk to age 80 years for BRCA1 and BRCA2 mutation carriers? Test your knowledge of ovarian cancer in our latest quiz.