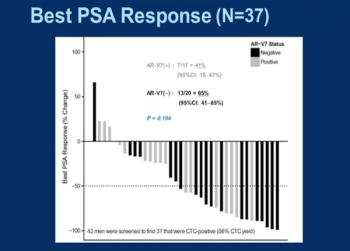
This slide show includes some of the top highlights from the 2015 ASCO Genitourinary Cancers Symposium, including a study that examined the risk of aggressive prostate cancer in testicular cancer survivors and more.
This slide show includes some of the top highlights from the 2015 ASCO Genitourinary Cancers Symposium, including a study that examined the risk of aggressive prostate cancer in testicular cancer survivors and more.

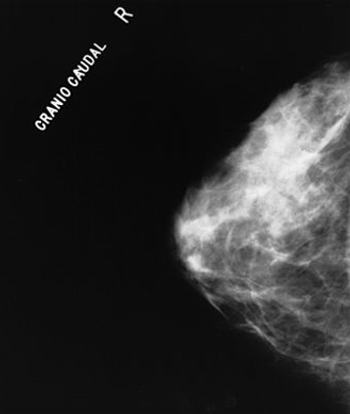
As part of our MBCC coverage we discuss MRI screening for breast cancer in patients who carry a BRCA mutation or have a first-degree relative who is a BRCA carrier.
A recent study found that radiation therapy was effective for the palliation of painful spinal metastases in patients with hepatocellular carcinoma.
A new study suggests that cancer patients do not often request unnecessary and sometimes costly tests or treatments.

This slide show highlights recent studies that examined coffee consumption as it relates to cancer risk, including melanoma, breast and liver cancers, and more.
A new study finds that childhood cancer survivors are at risk for pituitary hormone deficiencies after radiotherapy treatment to the head.

The best, most likely, and worst-case prognostic framework is a helpful tool for discussing median survival with patients in a way that enables them to make sense of the data.

CMS has launched a new multi-payer cancer payment model that reimburses oncologists for episodes of care surrounding chemotherapy treatment, part of a larger effort by the agency to reward physicians based on quality rather than quantity of care.

Women in routine gynecologic care expressed willingness to extend screening intervals and use cytology alone or Pap-HPV cotesting if recommended by a physician.
An inhibitor of osteoclast formation can stop the proliferation of dormant tumor cells that in some breast cancer survivors turn into bone metastases.
Conservative management of cervical intraepithelial neoplasia (CIN) grade 2 is an appropriate treatment option for women aged 25 years and younger.
Researchers have identified eight specific physical signs associated with death within 3 days, which can help clinicians and families in making care decisions.

I do not want politicians passing laws to tell us how to practice. The legislative process cannot keep pace with changes in medicine.
In this interview we discuss how patient adherence to the American Cancer Society’s cancer prevention guidelines affects cancer risk and mortality.

The benefit of hypofractionated radiotherapy for women receiving breast-conserving therapy for early-stage breast cancer is becoming more apparent.
Adding molecular breast imaging to mammography resulted in a fourfold increase in invasive breast cancer detection rates in women with dense breasts.

This slide show includes some of the highlights from the 2015 ASCO Gastrointestinal Cancers Symposium, including a study that linked vitamin D levels to colorectal cancer outcomes, positive results in pancreatic cancer with a new targeted agent, and more.

Socioeconomic factors are reducing the use of combined-modality treatment for early-stage Hodgkin lymphoma, despite its association with increased survival.

A history of hormonal contraceptive use in younger women for 5 years or more was found to be associated with a possible increased risk of glioma.
Hepatocellular carcinoma patients with baseline alpha-fetoprotein (AFP) levels greater than 400 ng/mL may derive greater benefit from second-line ramucirumab.
This one-act play features a patient, former smoker, navigating the CMS rules for lung cancer CT screening in a shared decision-making session with his doctor.

A delirious head and neck cancer patient does not have the capacity to make treatment decisions. Can we begin palliative radiation therapy without his consent?

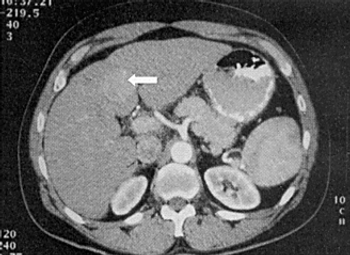
The radiologist could not have known exactly what was in store for me, but it obviously wasn’t good. Couldn’t he have dredged up even a nanoparticle of empathy

An FDA advisory panel unanimously endorsed EP2006, a biosimilar of filgrastim, a biologic used to treat neutropenia caused by chemotherapy treatment.
Women with bilateral malignant ovarian germ cells tumors may still have a good prognosis and may be able to maintain fertility with conservative treatment.
In a phase III trial, erlotinib performed no better than placebo when added to sorafenib in treatment-naive patients with advanced hepatocellular carcinoma.

Older men who received radiotherapy in addition to ADT had fewer deaths from their locally advanced prostate cancer compared with those treated with ADT alone.

Experts from ASCO and AACR have penned a statement for policymakers on the potential negative effects of e-cigarettes and other nicotine-deliveries electronics.
Adding radiotherapy to adjuvant chemotherapy in the ARTIST trial yielded similar results to chemo alone in patients with D2 lymph node-resected gastric cancer.

Adding an MRI to a mammogram improved the sensitivity of breast cancer screening in women 50 years of age or older who are BRCA mutation carriers.