

Expert Commentary on the Product Profile of Tislelizumab in Advanced Esophageal Cancer
Krystal Preston, PharmD, BCPS, discussed the use and administration of tislelizumab for patients with resectable or metastatic esophageal squamous cell carcinoma.


Krystal Preston, PharmD, BCPS

Krystal Preston, PharmD, BCPS, spoke about the use of tislelizumab-jsgr (Tevimbra) for patients with unresectable or metastatic esophageal squamous cell carcinoma. She highlighted specific adverse effects (AEs) observed with this drug and how it is showing promise in different settings and disease types.
Q / What is tislelizumab’s mechanism of action?
Preston / This is an anti–PD-1 antibody that binds to the PD-1 receptor and blocks interactions between PD-1 and its ligand PD-L1, releasing the PD-1 pathway–mediated inhibition in the immune response. When we bind the PD-1 receptor with its ligand found on T cells, it inhibits T-cell proliferation and cytokine production. Blocking PD-1 activity has resulted in decreased tumor growth in animal models in different studies.


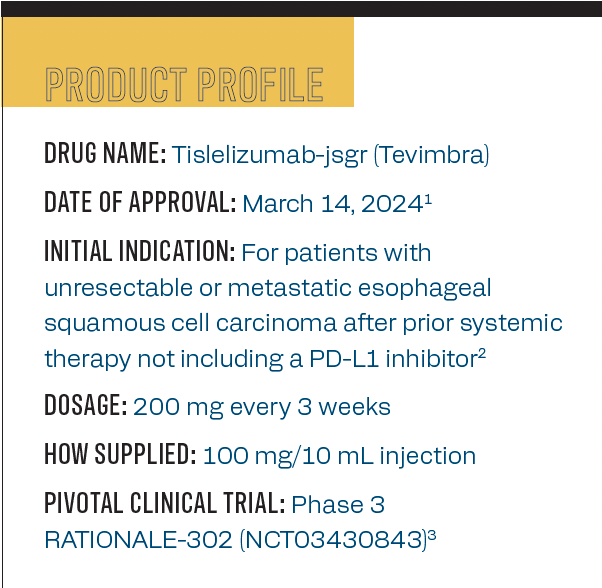
The product profile of tislelizumab.
Q / Are there any specific characteristics that may help identify patients who are most likely to benefit from tislelizumab therapy?
Preston / Currently, tislelizumab is a second-line therapy option that will most likely benefit patients who have advanced or metastatic esophageal squamous cell carcinoma, and patients who have progressed on first-line therapy.


DESIGN OF THE PHASE 3 RATIONALE-302 TRIAL
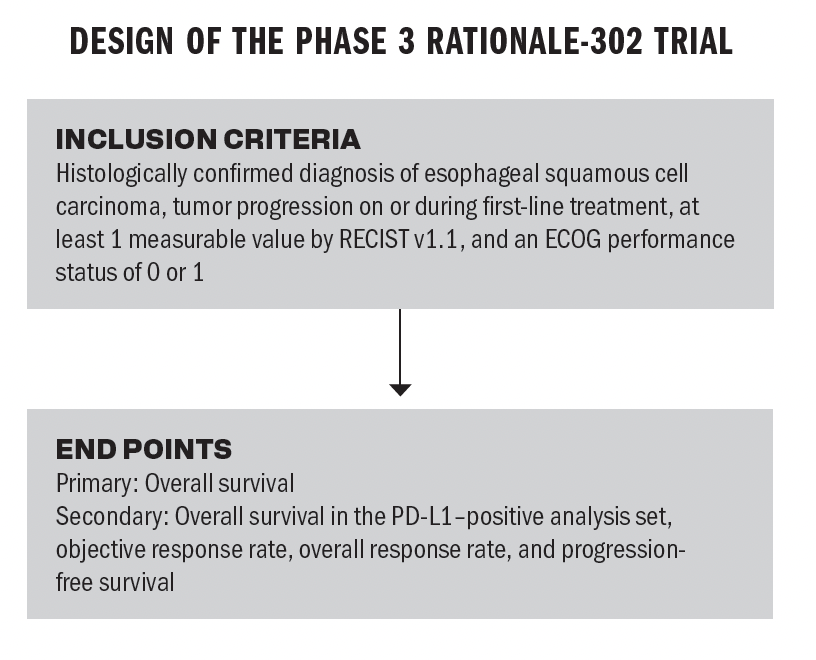
Q / RATIONALE-302 findings demonstrated an improvement in overall survival (OS). How is that significant in the context of treatment options available for unresectable or metastatic esophageal cancer?
Preston / It’s very significant. In fact, more studies have been done beyond RATIONALE-302. In terms of this study, the OS with tislelizumab was statistically significant and showed a clinically meaningful improvement compared with chemotherapy. OS with the tislelizumab group was 8.6 months vs 6.3 months in the chemotherapy group. These results are similar to other anti–PD-1 drugs that are indicated for esophageal squamous cell carcinoma.
However, in a more recent study, the phase 3 RATIONALE-306 trial [NCT03783442], tislelizumab plus chemotherapy demonstrated superiority over chemotherapy plus placebo. The OS was 17.2 months in the tislelizumab plus chemotherapy ground vs 10.6 months in the chemotherapy plus placebo group. That’s significant. We use tislelizumab right now in the second-line therapy space. With the most recent data, we see that it has the potential to be a contender in the first-line therapy space similar to other drugs in its class such as pembrolizumab and nivolumab.
Q / What are some of the most common AEs that are observed with tislelizumab, and how do they compare with other treatments for esophageal cancer?
Preston / Usually, first-line therapy for esophageal cancer involves chemotherapy; that’s our first-line option. When we get into second-line options, we now have other immunotherapies, and some of those immunotherapies are used first line now as well. In terms of the AEs, tislelizumab is similar to other PD-1 drugs for this particular cancer indication, but it’s still less than we see with chemotherapy. We have the standard metabolic effects like decreased sodium [levels], hypothyroidism, and increased serum glucose [levels]. We also see an increase in the liver enzyme [levels], specifically serum alkaline phosphatase. We also see hematological effects such as anemia and decreased platelet count. Other AEs would include gastrointestinal effects like abdominal pain, nausea, and vomiting. Additionally, [we see] fatigue, musculoskeletal pain, and cough. These are standard with the other drugs in this class.
Q / As with other targeted therapies, resistance may develop. What are some known potential resistance mechanisms associated with tislelizumab?
Preston / There are several potential immunotherapy resistance mechanisms that can impede the antitumor activity of these immunotherapy drugs. Some of these mechanisms include antigen deletion, T-cell dysfunction, increased immunity of immunosuppressive cells, and the alteration of ligand expression within tumor cells. Specific to PD-1 immunotherapies, it’s important to note that the nonpotential mechanisms of resistance involve the interaction between the Fc region of the drug and the Fcγ receptor on the macrophages of those tumor cells, which would induce phagocytosis. With tislelizumab and the RATIONALE-302 trial, it was noted that this particular anti–PD-1 monoclonal antibody was engineered to minimize binding of that Fc region to the Fcγ receptor. This is crucial when it comes to antitumor activity. The inability of the Fc region on the drug to bind with the Fcγ receptor on the tumor limits antibody-dependent phagocytosis. Therefore, we’re eliminating the resistance mechanism.
Q / Where do you see this agent headed?
Preston / Tislelizumab is currently FDA approved for resectable/metastatic esophageal squamous cell carcinoma but only in the second-line setting. Things are looking promising for tislelizumab, which is likely to receive more FDA-approved indications, and it is expected to be approved in the first-line setting in combination with chemotherapy, such as etoposide and carboplatin. This approval will be based on the RATIONALE-306 trial [findings].
It is also expected to be approved in the first-line [setting for] advanced gastric and gastroesophageal cancer, and that has the Prescription Drug User Fee Act date of December 2024. There are other disease states where tislelizumab is being studied as well, including hepatocellular carcinoma. The National Comprehensive Cancer Care Network guidelines have already approved it to be used as first-line therapy for hepatocellular carcinoma and for patients who are ineligible for resection transplant or local regional therapy. Tislelizumab is also being studied in urothelial carcinoma, Hodgkin lymphoma, and so many other types of cancer.
Q / Is there anything else you would like to highlight today?
Preston / Tislelizumab was approved in March as a second-line option for esophageal squamous cell carcinoma. It has the potential to gain approvals and treat some of the same cancers as its competitors, such as nivolumab [Opdivo] and pembrolizumab [Keytruda]. Based on its premier drug design that helps it to evade resistance mechanisms and with the new promising data, tislelizumab is a strong contender and is a premier cancer therapy option. This may even supersede the other drugs in this class in the future. There is a lot more to come with tislelizumab.
References
- BeiGene receives FDA approval for Tevimbra for the treatment of advanced or metastatic esophageal squamous cell carcinoma after prior chemotherapy. News release. BeiGene. March 14, 2024. Accessed July 17, 2024. https://shorturl.at/bzZ37
- Tevimbra. Prescribing information. BeiGene; 2024. Accessed July 17, 2024. https://shorturl.at/czr6Z
- Shen L, Kato K, Kim SB, et al. RATIONALE 302: randomized, phase 3 study of tislelizumab versus chemotherapy as second-line treatment for advanced unresectable/metastatic esophageal squamous cell carcinoma. J Clin Oncol. 2021;39(suppl 15):4012. doi:10.1200/JCO.2021.39.15_suppl.4012





Newsletter
Stay up to date on recent advances in the multidisciplinary approach to cancer.









The Proper Ways to Identify and Use ADCs in Breast Cancer Subtypes
June 29th 2025Deciding when to use immunotherapy and how to utilize antibody-drug conjugates are complicated processes that require multidisciplinary collaboration to ensure that all patients with breast cancer receive appropriate and efficient care.


