
The community oncology practice is the nation’s headquarters in the war on cancer. Eighty-five percent of all cancer patients receive their treatment in local community oncology practices.
The community oncology practice is the nation’s headquarters in the war on cancer. Eighty-five percent of all cancer patients receive their treatment in local community oncology practices.
We need to understand each patient’s cancer and its microenvironment well enough to develop targeted treatments that will kill the tumor the first time-for if we let it escape, 70 years of prostate cancer research teaches us that our job will only get harder.
Although high-level evidence is lacking, the existing literature indicates that select men with lymph node–positive prostate cancer benefit from local therapy.
There has never been a referendum on IL-2. True, in the era of paradigm-shifting therapies, IL-2 may be overlooked at times, but it must not be excluded from the conversation.
Palliation is a laudable concept and an important goal in the therapy of all patients with malignant disease. Unfortunately, in the current day and age, the adjective “palliative” is being used in a derogatory manner that suggests palliation of suffering somehow lessens the importance or impact that such a therapy has upon individuals with the disease.
By inhibiting inflammatory cytokines and controlling the signs and symptoms of myelofibrosis, the patient’s body condition improves as the disease is kept under good control. Ultimately, prolonged exposure of a patient with myelofibrosis to ruxolitinib at a clinically effective dose results in prolongation of the his or her life.

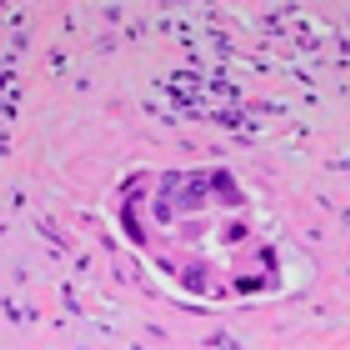
Surgery is the mainstay of treatment for localized soft-tissue sarcoma (STS). It consists primarily of resection of the tumor along with a cuff of surrounding healthy tissue. In limb and trunk wall sarcomas, this basically implies resection of the surrounding soft tissues, which are mainly muscles, subcutaneous fat, and skin.[1] In the retroperitoneum, this necessarily should imply resection of adjacent viscera, even when they are not overtly involved.[2] This is the only way to avoid/minimize the presence of tumor cells at the cut surface (ie, positive microscopic surgical margins). Positive microscopic surgical margins are associated with a higher risk of local failure, distant metastases, and death.[3-6] Moreover, for STS located at critical sites, such as retroperitoneal sarcoma (RPS), positive surgical margins may have a direct impact on survival, favoring the development of inoperable local recurrences.[7] Indeed, unlike with STS arising in the extremities and trunk wall, local control in RPS poses a significant challenge and remains the leading cause of death, particularly in patients with low- to intermediate-grade tumors-roughly 75% of all cases.[8-13] Extending the resection to adjacent uninvolved viscera for primary RPS is the only way to minimize the presence of microscopic surgical margins and hence maximize the chance of cure. In essence, this strategy should often include ipsilateral nephrectomy and colectomy; locoregional peritonectomy and myomectomy (partial/total) of the muscle of the lateral/posterior abdominal wall (usually the psoas) (see Figure); splenectomy and left pancreatectomy, for tumors located on the left upper side; occasionally pancreaticoduodenectomy or hepatectomy, for tumors located on the right side; and vascular and bone resection only if vessels/bone are overtly infiltrated.[2]

Recently controversy has emerged regarding the extent of resection that constitutes optimal surgical management of retroperitoneal soft-tissue sarcoma.
The patient is an otherwise healthy 45-year-old female who presented to her primary care physician with 6 weeks of increasing left upper quadrant abdominal pain with radiation to the back. She underwent an abdominal ultrasound, which revealed a large cystic abdominal mass.
Unfortunately, although agents in the pipeline each extend life, none are curative. Therefore, physicians who investigate and treat mCRPC have two paths they can follow to further improve outcomes.
A 40-year-old woman with no significant family history of cancer came to me for a second opinion about her widely metastatic infiltrating gastric cancer.
Ultimately, as agents in both VEGF-targeted and immunotherapy classes with lower toxicity rates are developed, questions of combination and sequence will inspire clinical investigations of strategies that, it is hoped, will maximize both the quantity and quality of life for patients with RCC. Melanoma therapy drug development continues to lead the way with regard to what is therapeutically possible with immunotherapy-and suggests that HD IL-2 continues to be relevant in today’s treatment landscape.
Node-positive prostate cancer without distant metastases (T any, N+, M0) currently is encountered rarely, primarily because of the shift to diagnosis at earlier stages, a result of widespread PSA testing.

In this article, we provide updated data on ruxolitinib therapy for patients with myelofibrosis and offer expert opinion on the appropriate use of this agent in the community practice.
In this review, we focus on the testosterone/androgen receptor pathway that is being targeted with potent new agents; we also discuss other important alternative biologic pathways that have given rise to new therapeutics that may attenuate prostate cancer growth, survival, and propagation.
The “experts” should maintain a stringent standard regarding what merits further development and reconsider carefully and critically the available data before committing to PARP inhibition, attacks on the PI3K pathway, and vasoactive agents in prostate cancer.
Current evidence for the management of lymph node–positive prostate cancer suggests both a disease-control and survival benefit to systemic ADT plus surgery and radiation.

In this review, we examine the currently approved options available for these disease processes, including the newer agents and selected combinatorial approaches under investigation, and we attempt to identify the role of high-dose IL-2 in the context of current clinical practice.