
|Articles|March 1, 2018
Quiz: Best Second-Line Tx for Metastatic Lung SCC and Crohn Disease?
Author(s)Mehmet Sitki Copur, MD
Are there special second-line considerations for an SCC lung patient with a history of Crohn disease who progressed on first-line carboplatin and gemcitabine? Can any pretreatment tests be deferred for a patient with a history of heavy smoking and a single solitary nodule found on his CT chest scan? Take this multiquestion quiz to find out.
Advertisement
Are there special second-line considerations for an SCC lung patient who progressed on first-line carboplatin and gemcitabine? Can any pretreatment tests be deferred for a patient with a history of heavy smoking and a single solitary nodule found on his CT chest scan? Take this multiquestion quiz to find out.
Question 1
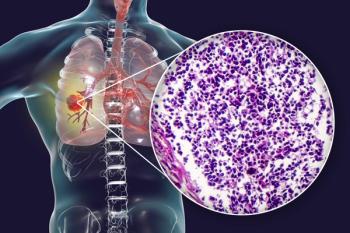
A 65-year-old man is being evaluated for second-line systemic treatment of his metastatic squamous cell carcinoma of the lung, which has progressed after six cycles of first-line therapy with carboplatin and gemcitabine. The patient continues to have an excellent performance status and no additional major medical issues other than a history of Crohn disease.
Answer
E.Docetaxel plus ramucirumab.
Given the patient's history of autoimmune colitis, treatment with nivolumab (A) may not be the safest choice. Prior platinum-based combination therapy makes combination treatment with carboplatin plus albumin-bound paclitaxel (B, C) less likely to be effective. In addition, bevacizumab (C) may not be safe to use in patients whose tumors have squamous cell histology. Single-agent treatment with docetaxel (D) is inferior to treatment with docetaxel plus ramucirumab, based on data from the REVEL trial.[1] Therefore, E is the appropriate choice.
Reference
1. Garon EB, Ciuleanu TE, Arrieta O, et al. Ramucirumab plus docetaxel versus placebo plus docetaxel for second-line treatment of stage IV non-small-cell lung cancer after disease progression on platinum-based therapy (REVEL): a multicentre, double-blind, randomised phase 3 trial. Lancet. 2014;384:665-73.
Question 2
A 68-year-old man with a history of heavy smoking was found to have a 2.5-cm solitary nodule on his CT scan of the chest. CT scans of the patient’s abdomen and pelvis did not show any other sites of disease. A CT-guided biopsy of this lesion revealed an adenocarcinoma.
Answer
D.Magnetic resonance imaging (MRI) of the brain, with contrast.
The patient has clinical stage T1bN0M0 stage IA non-small-lung cancer. If the rest of the work-up does not reveal any other site of disease and it remains as stage IA, then MRI of brain may not be needed. MRI of the brain is necessary for patients with stage II and IIIA disease, and optional for those with stage IB disease.[1]
Reference
1. NCCN Guidelines Version 4.2018. Non-Small-Cell Lung Cancer.
Question 3
A 58-year-old white male heavy smoker with recent prolonged coughing had a chest x-ray procedure that revealed a right upper lung nodule. Work-up with CT of the chest and upper abdomen and a CT-guided biopsy of the lung lesion revealed a 3.5-cm right upper lobe small-cell carcinoma. Further work-up with positron emission tomography/CT and brain imaging was negative.
Answer
D.Pathologic mediastinal staging with mediastinoscopy, mediastinotomy, endobronchial or esophageal US-guided biopsy or video-assisted thoracoscopy.
This patient has presented with clinical stage I (T1N0) lung cancer. Prior to resection, all patients should undergo mediastinoscopy or other surgical mediastinal staging to rule out occult nodal disease.[1]
Reference
1. NCCN Guidelines Version 3.2017. Small Cell Lung Cancer.
Question 4
A 72-year-old man with a history of heavy smoking presents with a 6-cm right upper lobe primary lung mass and metastatic lesions involving his liver and brain. Biopsy of liver lesion is consistent with small cell lung cancer. He is currently asymptomatic.
Answer
B.Systemic chemotherapy followed by whole brain RT.
Since this patient is asymptomatic, systemic treatment followed by radiation to the brain is the most appropriate next step.[1]
Reference
1. NCCN Guidelines Version 3.2017. Small Cell Lung Cancer.
Question 5
Answer
B.PD-1 has two ligands which are expressed on a wide range of immune effector cells but not on tumor cells.
PD-1 has two ligands, PD-L1 and PD-L2, which are expressed on both immune effector cells and on tumor cells.
Advertisement
Related Content
Advertisement



















































Advertisement
Advertisement
Trending on CancerNetwork
1
FDA Accepts NDA for Daraxonrasib in Pretreated Metastatic Pancreatic Cancer
2
RASolute 302 and the Future of Pancreatic Cancer Treatment: Paul Oberstein, MD, on the KRAS Breakthrough
3
Mapping the Full CAR T-Cell Journey in DLBCL From Referral to Survivorship
4
Balancing Oncologic Outcomes With Patient Priorities in Prostate Cancer Care
5