

Recap: Treatment Options for Patients With HER2-Positive Breast Cancer and Brain Metastases
A panel of experts in breast oncology builds a lively discussion on evolving approaches in the management of HER2+ metastatic breast cancer, including key considerations for the treatment of patients with brain metastases.

At an Around the Practice® presentation hosted by CancerNetwork®, specialists in breast cancer management discussed treatment options for patients with HER2-positive breast cancer and brain metastases. The panel was led by Erika P. Hamilton, MD, director of the Breast Cancer and Gynecologic Cancer Research Program at Sarah Cannon Research Institute at Tennessee Oncology in Nashville; Ryan T. Jones, MD, MBA, a radiation oncologist at Tennessee Oncology; Rita Nanda, MD, director of the Breast Oncology Program, associate professor of medicine, and associate professor of the Comprehensive Cancer Care Research Center at the University of Chicago Medicine in Illinois; and Tiffany A. Traina, MD, attending physician, vice chair of Oncology in the Department of Medicine, and section head of the Triple Negative Breast Cancer Clinical Research Program at Memorial Sloan Kettering Cancer Center as well as associate professor of medicine at Weill Cornell Medicine in New York.


Case 1
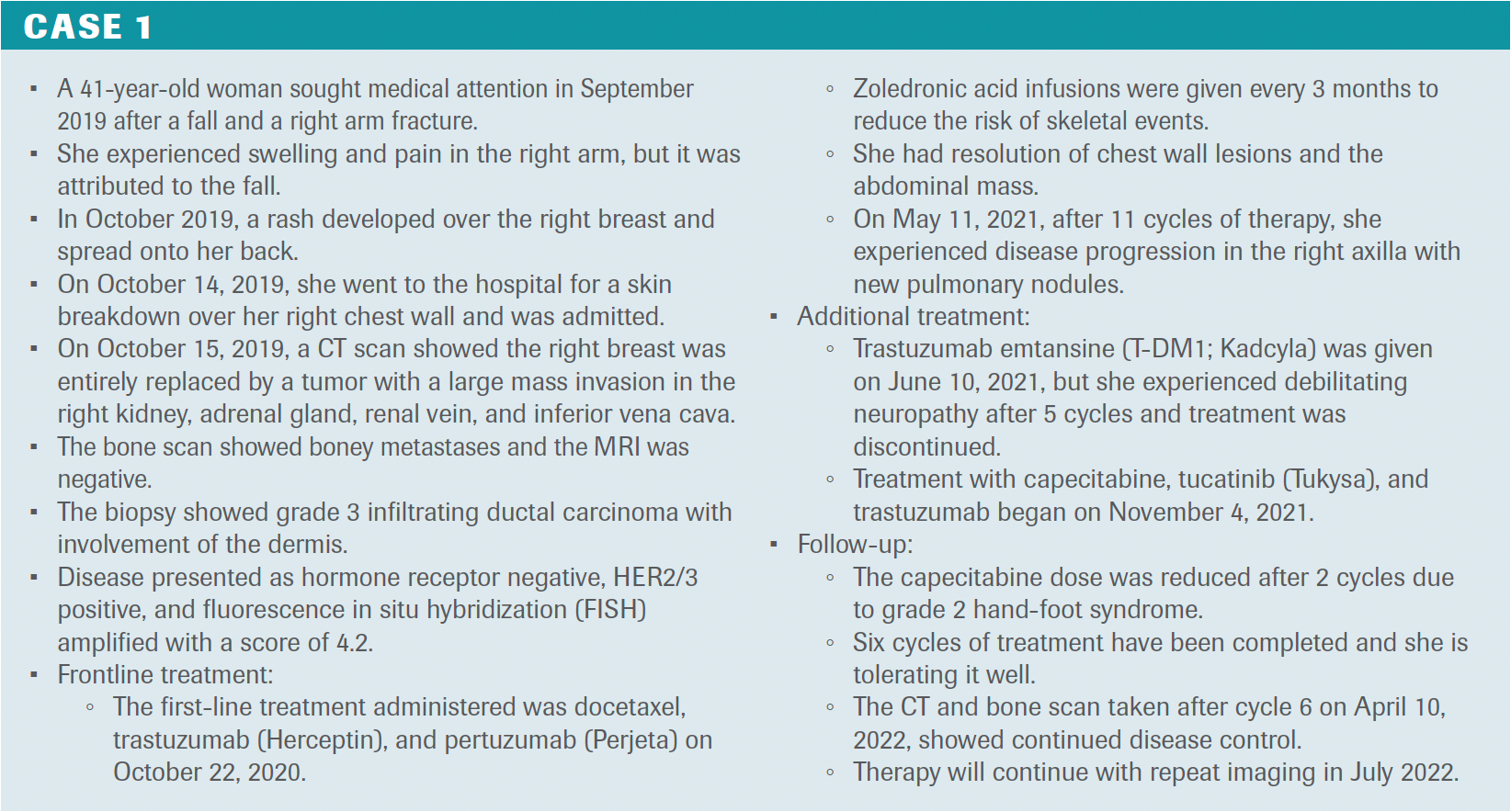
Hamilton: Can you discuss how you decide on first-line therapy for a patient with HER2-positive breast cancer?
Traina: The phase 3 CLEOPATRA trial [NCT00567190] regimen remains our first-line standard of care.1 CLEOPATRA compared docetaxel and trastuzumab with docetaxel, trastuzumab, and pertuzumab, and [the latter] was associated with about a 30% improvement in overall survival [OS]; at the time, it was probably the biggest incremental improvement in OS [57.1 vs 40.8 months; HR, 0.69; 95% CI, 0.58-0.82; P <.0001]. That established it as a first-line standard of care. Studies have also looked at paclitaxel with trastuzumab and pertuzumab. Guidelines would support taxane, trastuzumab, and pertuzumab in the first-line setting. Our expectations are that patients will have great benefits with that drug for a long time.
Hamilton: How many cycles of taxane do you normally consider before you stop administering it?
TRaina: Neuropathy is a potential toxicity with the taxanes, so there’s not an arbitrary number. Sometimes you hear 6 cycles and then dropping or treating to the point of maximal benefit. When toxicity develops, we’re inclined to drop the chemotherapy and keep the trastuzumab and pertuzumab as maintenance.
Hamilton: What about in the second-line setting?
Traina: We [are now lucky to] have multiple active agents in the second line and later. We have TKIs [tyrosine kinase inhibitors] and, as we’ve heard, tucatinib, capecitabine, and trastuzumab is a highly effective regimen. We have the antibody-drug conjugate [ADC] T-DM1 [ado-trastuzumab emtansine; Kadcyla] that’s been around for some time. [There are] newer data around the ADC trastuzumab deruxtecan [T-DXd; Enhertu]. We have data around a new engineered monoclonal antibody against HER2 called margetuximab [Margenza] as well as other TKIs like lapatinib [Tykerb] and neratinib [Nerlynx] that [are in use].
Hamilton: This patient received tucatinib in combination with capecitabine and trastuzumab in the third-line [setting]. What was your thought process when picking this regimen?
Nanda: She developed substantial neuropathy with T-DM1. It was very challenging to manage and took quite some time to resolve. Fortunately, it has [resolved], but we were looking for a regimen that wouldn’t be associated with neuropathy, would be easy to tolerate, and [was] an effective strategy. While she didn’t have brain metastases, she was at very high risk for them and it was very reasonable. This was prior to the availability of T-DXd.
Hamilton: This patient initially presented with a fracture. Would you recommend radiation therapy in the presence of bulky abdominal disease? How do you make those decisions?
Jones: I’m curious if it was a pathologic fracture from bone metastasis, but it sounds like it wasn’t. Then later, she was diagnosed with other boney metastatic sites. With respect to [whether] I would radiate the right axillary disease because of the edema, you’re right. We are there to help for troublesome areas, [such as] areas in the metastatic setting that are painful or bleeding and bothering some tissue. We deal with the management of lymphedema a lot in the local regional setting, such as after surgery [and] after surgery plus radiation, and in our preventive treatments and our therapeutic treatments of lymphedema and extremity. In [patients with metastatic disease], you want to minimize the time of significant lymphedema [to] try to prevent irreversible damage. We talk about stages [of the disease], whether it’s correctable by elevation and the degree of lymphedema of the extremity, but [it may] be very reasonable to deliver palliative radiation to this case to try to reduce that mass effect and improve the drainage for this patient.
Hamilton: What factors do you take into consideration when you’re choosing treatment for a patient with HER2-positive disease?
Nanda: We have so many exciting new therapies and there are many options. There isn’t necessarily just 1 way forward. We know that tucatinib has great CNS [central nervous system] activity from the [phase 2] HER2CLIMB trial [NCT02614794], and there’s a survival advantage even in those individuals who have brain metastases.2 I take that into account when I think about to whom I will recommend tucatinib, but I also have many patients who [have other concerns, such as not losing] their hair. They want to have hair for some time and they may like this idea of a convenient oral regimen. They’re only coming in once every 3 weeks for trastuzumab, and that can even be given subcutaneously. There are lots of reasons to consider tucatinib-based therapy. There’s the survival advantage. It’s very effective in brain metastases. Sometimes for patients, it’s a quality-of-life determination. While we have other therapies that are more effective than what we’ve historically had, there are many reasons to consider tucatinib-based therapy.
Hamilton: What do you think about the idea of delaying or preventing brain metastases?
Traina: It’s certainly hypothesis generating that we have some tools that might get us there because the development of brain metastases over the lifetime of a woman with HER2-positive breast cancer is unfortunately quite high. We are beginning to see a signal of certain drugs having great activity in the CNS; this has us hopeful that we can [be proactive about prevention by moving those drugs to an earlier line of therapy]. This is hypothesis generating [and] needs support from a clinical trial, but you can imagine that tools like tucatinib combined with other agents or as a single agent—perhaps moved up earlier—might help prevent the onset of brain metastases. Having good systemic control helps to minimize the development of brain metastases down the line as well.
Hamilton: How does radiation oncology contribute?
Jones: Our role is still central for brain metastases. We’re encouraged by improved, newer drug regimens that have more activity inside the CNS. I’m certainly biased being a radiation oncologist, but our role is still central. A lot more [patients have] HER2-positive or triple-negative [breast cancer] than [estrogen receptor]–positive, HER2-negative [breast cancer].
Hamilton: Can you outline other situations in which tucatinib may be used?
Nanda: A few ongoing trials are looking at adding tucatinib to ADCs. The HER2CLIMB-02 trial [NCT03975647] is looking at T-DM1 with or without tucatinib, and the HER2CLIMB-04 trial [NCT04539938] is looking at trastuzumab deruxtecan with tucatinib. We’re looking earlier now, even in postneoadjuvant therapy. In the early-stage setting for those patients who have not achieved a pathologic complete response to their standard neoadjuvant therapy, there’s the option to be randomized to T-DM1 with or without tucatinib in the CompassHER2 RD trial [NCT04457596]. [This trial may show whether we] can prevent brain metastasis for patients with early-stage breast cancer.
Hamilton: What about new agents [for HER2-positive breast cancer]?
Traina: We must keep in mind that many of these trials were designed in parallel before we had the data from other trials. As we’re trying to interpret the optimal sequencing of agents, a lot of this is unclear. As we’re incorporating ADCs, a big issue is trying to understand what the mechanism of resistance is when it does develop. Some of the novel agents that we’re seeing are other ADCs [targeting] HER2 but with different payloads. [It’s] important to emphasize that we have to understand mechanisms of resistance.

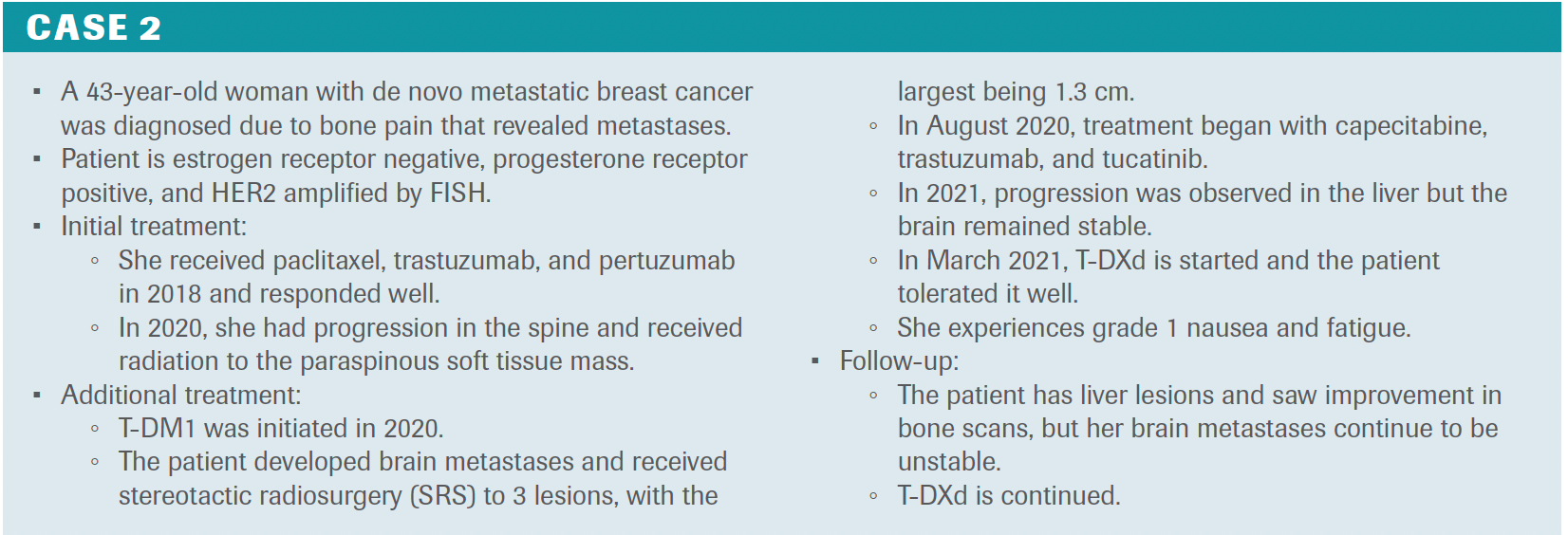
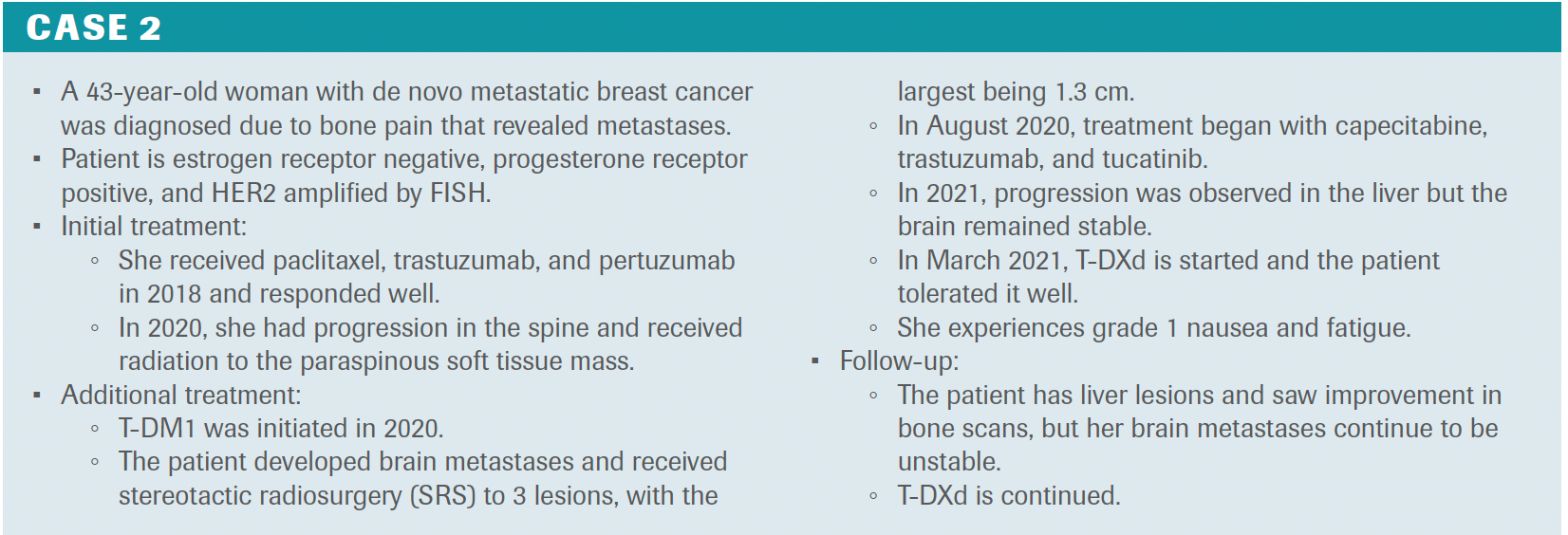
Hamilton: How might you have treated this patient? Is this case representative of a patient you see in clinic?
Nanda: I have seen patients like this. Most of our patients [present with] de novo metastatic disease now, so this is consistent with what I’ve seen. We know from the HER2CLIMB trial that patients with brain metastases have had regression of their brain metastases on tucatinib-based therapy. I had 2 patients who participated on that trial who went in with small brain metastases that regressed on therapy. I subsequently found that out after the fact when treatment was unblinded and [I learned that] they were [in the] tucatinib [arm]. Now, if I saw a patient like this, I might not do stereotactic radiosurgery; [I might] just treat with the HER2CLIMB regimen, see how it goes, and radiate if needed.
Traina: One [questionable] area [for me is when] she progressed in the CNS with these small lesions, what was happening extracranially? Today, guidelines would suggest that if everything else was quiet, we could just do a local therapy and then maintain that systemic treatment. Now, knowing the benefits of tucatinib, we all wonder if this is an opportunity to change up systemic therapy, hoping that we’ll get better CNS control. This is tricky and something that gets personalized. If the regimen is otherwise managed so well and our patients are feeling well, if our radiation colleagues can address those small spots, maybe we’re able to stretch systemic therapy longer before we need to make a change.
Hamilton: What evidence do we have for use of T-DXd in HER2-positive breast cancer, specifically around brain metastases?
Nanda: It’s exciting when we think [about newer therapy options, knowing that] the vast majority of patients with metastatic HER2-positive breast cancer will develop CNS disease over their disease journey. It’s nice to know that we’ve got multiple options now that can result in response to systemic therapies. Some data now with T-DXd from the TUXEDO-1 trial [NCT04752059] and from the subgroup analysis of the DESTINY-Breast01 trial [NCT03248492] demonstrate that these agents have substantial intracranial responses in the 50% to 70% range, even for individuals who have previously received radiation therapy.3,4 It’s exciting to see that [we now have more than] just radiation; we’ve got systemic therapies that adequately penetrate the CNS to help control disease.
Hamilton: How do you decide on SRS vs whole brain radiation therapy?
Jones: There are a few key features for deciding on SRS vs whole brain [radiation]. The performance status of the patient [and] extracranial control or patterns [of progression are important]. If I see it flourishing outside the brain, it gives me pause over what I will see in a few months if I’m just addressing these lesions locally. Still, the overall theme at present is avoiding whole brain [radiation] at all costs. If we’re going to do it, can we justify a hippocampal sparing or so-called hippocampal avoidance style to try to minimize long-term cognitive effects or the incidence of significant fatigue after whole brain radiation?
This idea of micrometastatic disease is that we can reliably help with bigger [areas of disease by] working together. I’m encouraged that we [may be able to] justify radiosurgery in a higher number of lesions, but it’s also limited by technology and what’s in your region. Some might say that the radiation oncologist they work with doesn’t routinely do this for more than 5 lesions. It could be technology is limiting that provider because it takes some advanced equipment to treat many lesions in a time that’s practical for the clinic.
Hamilton: If brain metastases progress or if there are new lesions, how do you decide when you continue with SRS vs whole brain radiation?
Jones: The first few MRIs after surgery can be tricky as to whether you’re seeing transient pseudoprogression, which we see with some agents. I’m curious how these therapies might play together. We’ve seen some in the setting of radiosurgery with immunotherapy, suggesting that we’re improving response by delivering the 2 together. I take pause with subtle changes on the first MRI and watch closely. Let’s not jump to surgery or radiosurgery and repeat if the patient is asymptomatic. Certainly, we’ll use steroids or try to help symptoms. I do [continue to use SRS] if possible. I’m a believer in it, if the number of lesions, disease pattern, and performance status of the patient can justify it.
Hamilton: This patient went on to receive T-DXd. What adverse effects are associated with T-DXd?
Nanda: Patients will certainly talk about hair loss. We know scalp cooling isn’t generally effective here. I’ve seen nausea with T-DXd, although it’s manageable. I’ve had 1 patient who struggled with it so I would bring her back periodically for [intravenous] fluids, but then over time it just got better. You come in once every 3 weeks with T-DXd having more fatigue, more nausea, as well as hand-foot syndrome and diarrhea.
Hamilton: How do you treat a patient who has progressed on T-DXd?
Traina: Clinical trials are always a great option. It depends on what these patients have previously seen because with DESTINY-Breast03 data, T-DXd is in that second-line space now. Some of our high-risk patients may have already received T-DM1 or pertuzumab in early-stage disease. In second-line, if they’ve received tucatinib, I’m giving T-DXd afterward. If they’ve received T-DXd in the second line, tucatinib remains a great option to reach for. Then we still have agents like margetuximab plus chemotherapy. We have other TKIs like lapatinib plus capecitabine and neratinib plus capecitabine.
Hamilton: What do we need to do moving forward?
Nanda: I’m really excited about the ADCs in development. We need to understand the mechanisms of resistance to these agents, how to sequence them better, and how to sequence all of these amazing therapies in the most strategic way so that we can help women live longer and better and avoid brain metastases. We’re doing such a great job controlling visceral disease; [however], brain metastasis still become an issue. Again, to see 2 amazing regimens that are associated with the intracranial response is exciting.
References
- Swain SM, Miles D, Kim S-B, et al; CLEOPATRA Study Group. Pertuzumab, trastuzumab, and docetaxel for HER2-positive metastatic breast cancer (CLEOPATRA): end-of-study results from a double-blind, randomised, placebo-controlled, phase 3 study. Lancet Oncol. 2020;21(4):519-530. doi:10.1016/S1470-2045(19)30863-0
- Curigliano G, Mueller V, Borges V, et al. Tucatinib versus placebo added to trastuzumab and capecitabine for patients with pretreated HER2+ metastatic breast cancer with and without brain metastases (HER2CLIMB): final overall survival analysis. Ann Oncol. 2022;33(3):321-329. doi:10.1016/j.annonc.2021.12.005
- Bartsch R, Berghoff AS, Furtner J, et al. Trastuzumab-deruxtecan (T-DXd) in HER2-positive breast cancer patients (pts) with active brain metastases: primary outcome analysis from the TUXEDO-1 trial. Ann Oncol. 2022;33(suppl 3):S194-S223. doi:10.1016/annonc/annonc894
- Jerusalem GHM, Park YH, Yamashita T, et al. Trastuzumab deruxtecan (T-DXd) in patients with HER2+ metastatic breast cancer with brain metastases: a subgroup analysis of the DESTINY-Breast01 trial. J Clin Oncol. 2021;39(15 Suppl):abstr 526. doi:10.1200/JCO.2021.39.15_suppl.526





Newsletter
Stay up to date on recent advances in the multidisciplinary approach to cancer.







Treatment Combinations for HER2-Positive Breast Cancer
March 7th 2013As part of our coverage for the 30th Annual Miami Breast Cancer Conference, we bring you an interview with Dr. Mark Pegram, director of the breast cancer program at the Stanford Women’s Cancer Center and codirector of the molecular therapeutics program. Dr. Pegram will be discussing the potential for novel HER2 combination therapies at the conference.



