Evaluation and Management of Testicular Cancer After Late Relapse
The clinical quandary by Langer et al discusses a contralateral late relapse of the original right nonseminomatous germ cell tumors.
Abstract
A 41-year-old man presented to his primary care physician with a 1-month history of left neck adenopathy in the context of a history of nonseminomatous germ cell tumors (NSGCTs). In 2011, the patient was treated for stage IB (T2N0M0S0) right-sided NSGCTs of the testis, which were 95% embryonal and 5% yolk sac tumors. He underwent a right radical orchiectomy and was followed until 2022 without recurrence.
In the work-up for his adenopathy, laboratory results for human chorionic gonadotropin, lactate dehydrogenase, and α-fetoprotein were normal. CT scans confirmed clustered enlarged lymph nodes in the left lower spinal accessory posterior triangle, enlarged left lower neck lymph nodes, and several foci of enlarged left retroperitoneal periaortic lymph nodes. Fine needle aspiration of a left neck lymph node identified malignant tumor cells. A left neck dissection showed embryonal carcinoma in 12 of 28 nodes. Immunostaining showed the tumor cells were positive for SALL4 and CD30 but negative for CD117.
This patient likely had a contralateral late relapse of his original right NSGCT after 11 years of remission. The patient’s original cancer was on the right side, with recurrence surrounding the aorta on the contralateral side, representing an atypical pattern of spread.
Case Report
A 41-year-old Asian man presented to his primary care physician (PCP) in January 2023 with a 1-month history of left neck adenopathy in the context of a prior history of nonseminomatous germ cell tumors (NSGCTs). In 2011, the patient was treated for stage IB (T2N0M0S0) right-sided NSGCTs of the testis.
The patient had multifocal tumors, 2.9 cm and 1.3 cm in greatest dimension, which were 95% embryonal and 5% yolk sac tumors. He underwent a right radical orchiectomy and was followed until 2019 under surveillance without evidence of recurrence. In July 2022, the patient had normal tumor markers and in September 2022 had normal CT scans. The patient is married and a nonsmoker, with no alcohol history and no history of undescended testis or infant surgery. At the time of this visit with his PCP to discuss the left neck adenopathy, he had no recent history of an upper respiratory infection and denied bladder changes, bleeding or bruising, bowel changes, cough or hoarseness, fatigue, night sweats, weight loss, pain, and persistent fever.
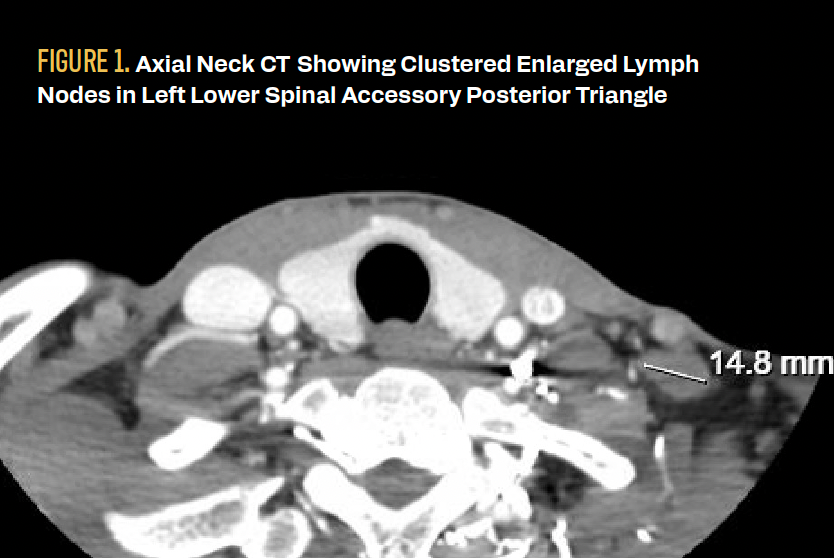
Soft tissue ultrasound in January 2023 revealed enlarged left neck lymph nodes that could be either pathological or reactive, with a decrease or loss of fatty hilum. The largest lymph node was 1.8 × 1 × 1.5 cm. His laboratory results were normal with a human chorionic gonadotropin (hCG) level of less than 1 IU/L, lactate dehydrogenase (LDH) level of 164 U/L, and α-fetoprotein (AFP) level of 2.9 μg/L; neoplastic syndrome was not indicated. A subsequent CT scan of his neck 3 weeks later confirmed clustered enlarged lymph nodes in the left lower spinal accessory posterior triangle, with left lower neck lymph nodes measuring up to 1.6 cm and a paratracheal cystic lesion measuring 1.8 cm in greatest dimension (Figure 1).


FIGURE 1. Axial Neck CT Showing Clustered Enlarged Lymph Nodes in Left Lower Spinal Accessory Posterior Triangle
A CT scan of the chest/abdomen/pelvis 1 month after the CT scan of the neck confirmed the neck lymphadenopathy as well as several foci of left retroperitoneal periaortic lymph nodes that were enlarged, all less than 2 cm in greatest dimension (Figure 2).


FIGURE 2. Coronal CT Abdomen and Pelvis Showing Several Foci of Periaortic Lymphadenopathy

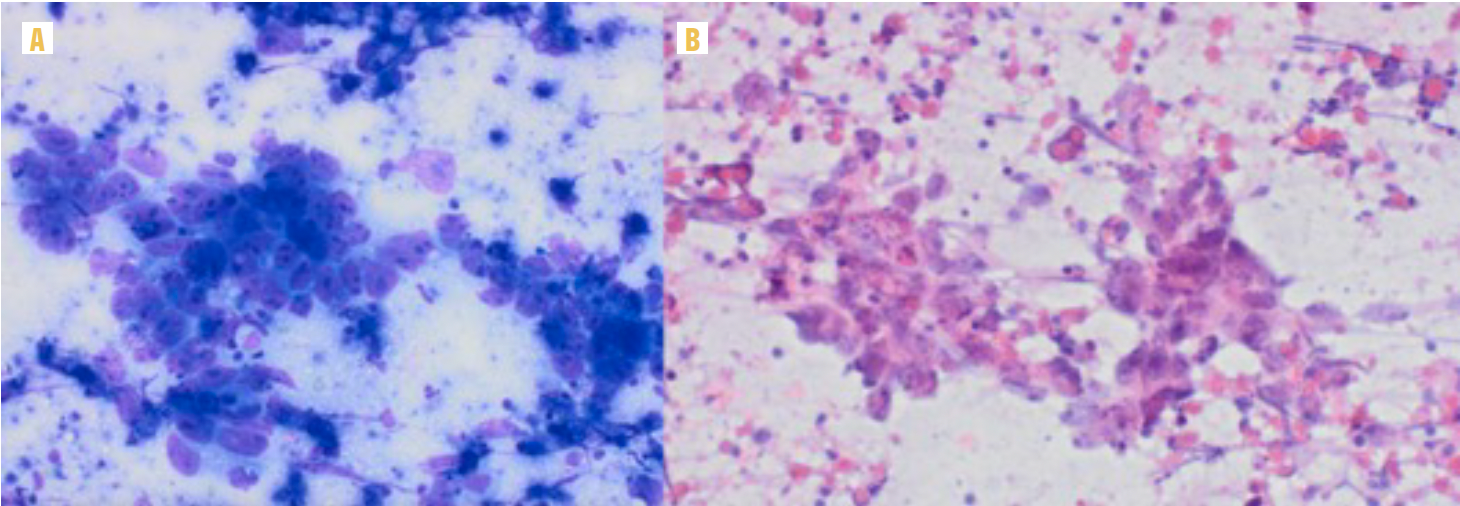
Scrotal ultrasound at this time showed diffuse left testis microlithiasis that was otherwise normal, and tumor markers were notable for an LDH level of 303 U/L (elevated), AFP level of 3.4 μg/L, and an undetectable hCG level. Initial fine needle aspiration (FNA) of a left neck node identified malignant tumor cells with clusters of pleomorphic malignant cells in a background of necrotic debris, with insufficient material for further characterization (Figure 3).

 Diff-Quik stain (×20): Pleomorphic malignant cells with large irregular nuclei, coarse chromatin, prominent irregular nucleoli, vacuolated cytoplasm, and indistinct cell borders (syncytial growth pattern). (B) Papanicolaou stain (×20): Syncytial cluster of pleomorphic malignant cells with coarse chromatin and prominent nucleoli in a background of necrotic debris.")
FIGURE 3. Staining Results (A) Diff-Quik stain (×20): Pleomorphic malignant cells with large irregular nuclei, coarse chromatin, prominent irregular nucleoli, vacuolated cytoplasm, and indistinct cell borders (syncytial growth pattern). (B) Papanicolaou stain (×20): Syncytial cluster of pleomorphic malignant cells with coarse chromatin and prominent nucleoli in a background of necrotic debris.
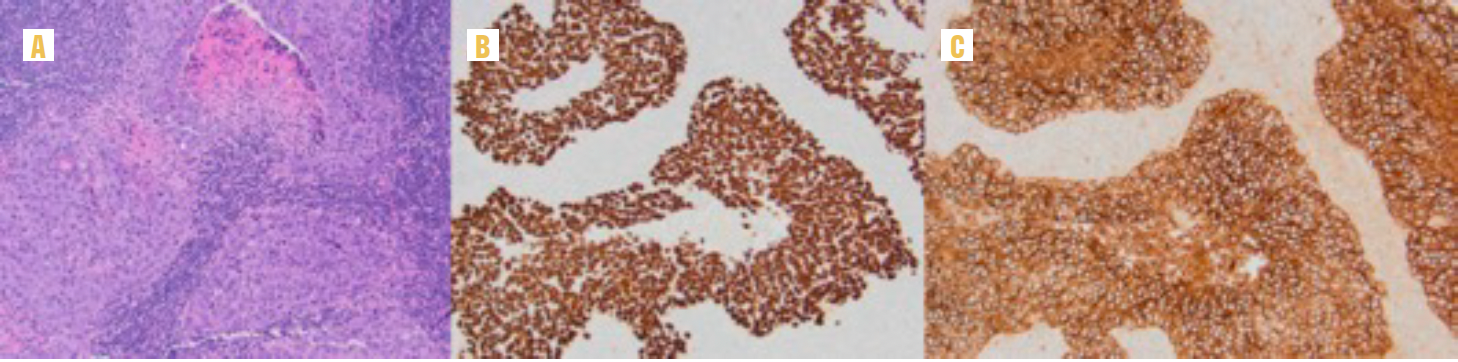
Four months after his first presentation at his PCP office, the patient underwent left neck dissection with pathology showing embryonal carcinoma in 12 of 28 nodes, with a maximum nodal size of 2.5 cm in greatest dimension. Immunostaining showed the tumor cells were positive for SALL4 and CD30 and negative for CD117 (Figure 4).

 Hematoxylin and eosin stain (×100): Solid nests of malignant cells with synthetical growth pattern, prominent nucleoli, and tumor necrosis in a background of lymphoid tissue. (B) SALL4 immunostain stain (×100): Strong nuclear positivity. (C) CD30 immunostain stain (×100): Strong and diffusely membranous positivity.")
FIGURE 4. Additional Results (A) Hematoxylin and eosin stain (×100): Solid nests of malignant cells with synthetical growth pattern, prominent nucleoli, and tumor necrosis in a background of lymphoid tissue. (B) SALL4 immunostain stain (×100): Strong nuclear positivity. (C) CD30 immunostain stain (×100): Strong and diffusely membranous positivity.
What is the likely diagnosis based on the presenting illness and initial work-up?
Introduction
Testicular cancer is the most common cancer in young men, with 95% of testicular cancers being germ cell tumors (GCTs).1 Within testicular GCTs, nonseminomas make up approximately 40% and the rest are seminomas.1 The majority of patients with NSGCT are cured. However, late relapse of this cancer has been well documented and researched.1
Late relapse of testicular cancer is defined as occurring more than 2 years after initial diagnosis and surveillance or complete response to treatment.1 In recent research, up to 7% of patients with NSGCT have had a late relapse, which is more common than previously thought.1,2 The median number of years for late relapse of all testicular cancers is 6 years (range, 2-32).1,3 In a 1994 Urologia Internationalis article, researchers described late relapse of NSGCT after orchiectomy and retroperitoneal lymph node dissection (RPLND) 40 months after surgery, with the only marker for recurrence being elevated AFP.4 Reports of late relapse of NSGCT are found throughout the literature and may be on the rise.
In this report, we review a patient with a rare presentation of contralateral late-onset relapse of NSGCT after 11 years in remission. This case is unique in that the patient not only falls into the category of late relapse but also far surpasses the average relapse timeline of 6 years. Additionally, his presenting symptom was left neck adenopathy, with no other initial signs or symptoms of recurrence.
Late Relapse and Contralateral Retroperitoneal Recurrence
From the findings of the left neck dissection, the morphology and immune profile support the diagnosis of embryonal carcinoma (answers B, C, and E are incorrect).Notably, the histological profile cannot reveal whether this is a late relapse or a secondary primary tumor. The lack of a discrete mass on scrotal ultrasonography, normal semen parameters, and normal gonadal function lead us to believe a burned-out or regressed metastatic left primary is less likely. Nevertheless, the presence of microlithiasis in a patient with a history of GCT must be considered as a risk factor for GCT. The timing and pattern of this patient’s presentation are atypical for a NSGCT. Typically, we would expect right-sided tumors to primarily metastasize to the interaortocaval and paracaval lymph nodes. However, this patient had relapse in the para-aortic distribution and left supraclavicular region, which is more common in left-sided tumors.
For late relapses, clinical presentations vary, marked by serum tumor marker elevation, surveillance imaging, or symptoms. The most common place for testicular cancer to relapse is the retroperitoneum, making up 50% to 80% of relapses due to the shared embryology of the testis and kidney.1,3 Late relapse may be seen in supraclavicular nodes and rarely in cervical nodes.1 Researchers in a 2023 case study described an initial presentation of metastatic seminoma being neck/axillary lymphadenopathy.5 Our patients’ periaortic and neck lymph nodes do follow these possible sites of metastatic spread, yet they are contralateral to what would be expected.
When it comes to laterality, left-sided tumors typically metastasize to left para-aortic nodes, and right-sided tumors metastasize to interaortocaval lymph nodes and paracaval lymph nodes.1 It is important to note that because of the normal anatomical crossover of the abdominal lymphatics from right to left, a right-sided tumor can present with left para-aortic nodes, especially when bulky. However, this crossover is not extensively described in patients with late relapses.1
Although it is rare, this patient’s original right-sided NSGCT has spread to left periaortic lymph nodes, likely in part due to the right-to-left crossover of abdominal lymphatics. His left neck lymph node is likely also a consequence of this crossover.
In the context of his diffuse left-sided microlithiasis, there is a raised concern for a left-sided primary secondary GCT. Results of a meta-analysis published in 2010 showed that testicular microlithiasis may represent an elevated risk of a testicular GCT in patients who are high risk, such as those with a history of GCTs. However, this risk has not been proven to be higher than the risk in patients without findings of testicular microlithiasis, and overall, it is still poorly understood.6 Lastly, his paratracheal abnormality remains somewhat perplexing but has features suggesting it is a mediastinal cyst rather than a pathologic lymph node.
Based on the clinical presentation, results from the FNA, immunostains from the biopsy, imaging, and review of the historical data, it is likely that this patient has a contralateral late relapse of his original right NSGCT after 11 years of remission (answer A is correct). However, we cannot fully rule out a secondary primary GCT in the left testis with 100% certainty without a left radical orchiectomy (answer D is unlikely but cannot be ruled out completely). With the patient declining to undergo an additional surgery, the cause of his current cancer status may never be completely known.
Treatment
This patient had chemotherapy-naive late recurrence of NSGCT without evidence of teratoma or somatic transformation of teratoma in either the primary tumor from 2011 or supraclavicular lymph nodes. Reasonable options included chemotherapy, RPLND, or observation. The volume of involved supraclavicular lymph nodes and enlarged retroperitoneal lymph nodes made systemic therapy the most attractive option. Also, the retroperitoneal disease was small at this time, with a reasonable chance of regression with chemotherapy and avoidance of RPLND. Given that the patient had not been previously exposed to chemotherapy, the prognosis was optimistic. After a multidisciplinary discussion with the patient and shared decision-making, he completed 3 cycles of bleomycin, etoposide, and cisplatin. A CT scan of the chest/abdomen/pelvis taken 2 months after the patient completed chemotherapy showed that the retroperitoneal nodes had resolved and a 9-mm right paratracheal abnormality was present. This is the area where an 18-mm paratracheal cystic lesion was seen on the first neck CT after presentation with the neck mass. The waxing and waning of the paratracheal abnormality throughout chemotherapy again may signal that it is a cystic process. Three months later, the most recent CT scan of the chest/abdomen/pelvis found that the retroperitoneal lymphadenopathy was still resolved, a likely node measuring 1.1 × 0.7 mm between the aorta and the left adrenal had not significantly changed from prior exams, and the upper right paratracheal node appeared less conspicuous. Tumor markers continue to be negative.
When it comes to screening for relapse, CT surveillance is one of the best tools for identifying relapse at an early stage while also providing the opportunity for prognostics and early treatment.1 As we have described in this paper, late relapse can present in many ways, with asymptomatic recurrence and/or contralateral retroperitoneal disease, making identification and diagnosis difficult. Patients need at least annual follow-up evaluations throughout their lives to identify late relapse.2 That being said, some researchers have found that patients with stage I NCGCTs or seminomas do not need follow-up 5 years after remission.7 However, in a patient such as the one described in this paper, there are no exact guidelines due to his unique case and presentation. This patient continues to be followed every 4 to 6 months with CT scans and tumor markers.
Patient Perspective and Testimonial
The patient was amenable to being interviewed about his experience with cancer as a part of this paper. After the patient received his initial diagnosis and was treated in 2011, he felt “very lucky that after the removal of the testicle, all the cancer biomarkers went down” and there were no signs of metastasis; years of negative scans followed. The patient changed his lifestyle after his cancer diagnosis, improving his diet and using meditation to help cope throughout his cancer journey, returning every 1 to 2 years for CT scans and laboratory testing. In 2023 when he presented to his PCP with concerns of left neck adenopathy, he was not immediately concerned that it was related to his cancer. He emphasized that he “[didn’t] think the mass was related because [there was] no other sign; this was the only sign. I did not have weight loss; I did not have other things that I can think of that related to cancer.” His most recent scans and laboratory results had been negative.
The patient was an active participant in his care. He searched for answers, trying to understand his cancer and why it was such a unique case. The patient mentioned he had another physician at a renowned testicular cancer institution who believes his cancer is possibly a primary tumor on the left side, but for a definitive diagnosis, he would need a left orchiectomy and lifelong hormonal therapy, which he was not interested in. This further emphasizes that we cannot know with 100% certainty whether there is a left-sided primary secondary GCT in this patient. However, we can use our best clinical judgment to guide care and share this unique case to further medical knowledge on this topic.
The patient ended with a strong statement pointing out the same questions that brought our clinical team to write up this case: “The interesting thing is that usually the tumor cell migrates through the same side, but this case is special. We don’t know why it migrated to the other side. That’s why we are having this conversation today. Hopefully, my case can help later research to see what kinds of things we can learn from here.” The patient would like to tell all patients with cancer and readers that when it comes to a long journey with cancer, “Try not to stress out about everything; keep your mind calm.” He emphasized that although the surgical treatment and chemotherapy have been life-changing, family support and meditation also have been very helpful.
Discussion
Although late relapse of NSGCT is rare, it has been on the rise, likely in part due to better treatment options and long-term survival.1 Notably, this patient presented with late relapse after 11 years in remission with contralateral retroperitoneal disease. The patient’s original cancer was on the right side, with recurrence surrounding the aorta on the contralateral side, representing an atypical pattern of spread for NSGCT. Based on this patient’s rare presentation and other literature with findings of contralateral retroperitoneal recurrence, it is important to be aware of the variation and spectrum of relapse and how to better identify late relapse when we encounter it.
Outcome and Follow-Up
As of February 2024, the patient is recovering uneventfully from the acute toxicities of chemotherapy and is being followed by urology, oncology, and otolaryngology.
Corresponding Author
Aditya Bagrodia, MD
Associate Professor, Department of Urology
University of California San Diego
Suite 1-200, 9400 Campus Point Drive
La Jolla, CA 92037
Phone: (858) 657-7876
Email: Bagrodia@health.ucsd.edu
References
- Rutherford EE, Ferguson JL, Geldart TR, Mead GM, Smart JM, Tung KT. Late relapse of metastatic non-seminomatous testicular germ cell tumours. Clin Radiol. 2006;61(11):907-915. doi:10.1016/j.crad.2006.06.009
- Baniel J, Foster RS, Gonin R, Messemer JE, Donohue JP, Einhorn LH. Late relapse of testicular cancer. J Clin Oncol. 1995;13(5):1170-1176. doi:10.1200/JCO.1995.13.5.1170
- Efstathiou E, Logothetis CJ. Review of late complications of treatment and late relapse in testicular cancer. J Natl Compr Canc Netw. 2006;4(10):1059-1070. doi:10.6004/jnccn.2006.0088
- Bilgrami S, Chen L, Shafi N, Synnott V, Greenberg B. An unusual late relapse in pathologic stage I non-seminomatous germ cell tumor: case report and review of the literature. Urol Int. 1994;53(3):176-178. doi:10.1159/000282665
- Yohannan B, Omo-Ogboi A, Kachira JJ, Jafri SH. Metastatic seminoma presenting as neck and axillary lymphadenopathy in an elderly man. Proc (Bayl Univ Med Cent). 2023;36(3):395-397. doi:10.1080/08998280.2023.2167184
- Tan IB, Ang KK, Ching BC, Mohan C, Toh CK, Tan MH. Testicular microlithiasis predicts concurrent testicular germ cell tumors and intratubular germ cell neoplasia of unclassified type in adults: a meta-analysis and systematic review. Cancer. 2010;116(19):4520-4532. doi:10.1002/cncr.25231
- Shahidi M, Norman AR, Dearnaley DP, Nicholls J, Horwich A, Huddart RA. Late recurrence in 1263 men with testicular germ cell tumors. Multivariate analysis of risk factors and implications for management. Cancer. 2002;95(3):520-530. doi:10.1002/cncr.10691
Joanna L. Langner, MS
School of Medicine, University of California San Diego, La Jolla, CA, US
Frederick Millard, MD
Department of Medical Oncology, University of California San Diego, La Jolla, CA, US
Vera Vavinskaya, MD; Haiyan Zhang, MD
Department of Pathology, University of California San Diego, La Jolla, CA, US
Nuphat Yodkhunnatham, MD; Aditya Bagrodia, MD
Department of Urology, University of California San Diego, La Jolla, CA, US