




















































Nivolumab is safe and effective in patients with metastatic bladder cancer refractory to prior lines of platinum-based chemotherapy, according to findings from the open-label, phase I/II CheckMate 032 trial.
Bladder Cancer
Latest News
Advertisement
Advertisement

Results of the IMvigor210 clinical trial found that atezolizumab is effective in patients with locally advanced or metastatic cisplatin-ineligible urothelial carcinoma.
The higher incidence of bladder cancer in the Northeast in the last 50 years may be attributed to the presence of arsenic in the drinking water, according to a new study.

The FDA has granted accelerated approval to atezolizumab (Tecentriq) for the treatment of locally advanced or metastatic urothelial carcinoma-the most common type of bladder cancer.
A new study found that FGFR3 mutation status could be used to guide anti-FGFR3 therapy in bladder cancer, as the mutation is homogeneous in radical cystectomy specimens and cancer-positive lymph nodes.
Afatinib showed significant activity in a phase II trial of patients with metastatic platinum-refractory urothelial carcinoma, and patients with HER2 or ERBB3 alterations had significantly better outcomes.
The diabetes drug pioglitazone was associated with an increased risk for bladder cancer among patients with type 2 diabetes, according to the results of a new study.
The American Society of Clinical Oncology endorsed the European Association of Urology’s treatment guideline on muscle-invasive and metastatic bladder cancer.
The US Food and Drug Administration has accepted the priority application for atezolizumab (MPDL3280A), an investigational targeted agent for patients with locally advanced or metastatic urothelial carcinoma.
The addition of ramucirumab to docetaxel improved progression-free survival compared with docetaxel alone in a randomized phase II trial of patients with locally advanced or metastatic urothelial carcinoma.
The emergence of immune checkpoint inhibitors as effective cancer immunotherapy has effectively built a new “highway” connecting the promise of oncologic translational research to progress in treating advanced malignancies.

In this interview we discuss predictive biomarkers and response to immune checkpoint inhibitors for urothelial tumors, which include tumors of the bladder, ureters, and the renal pelvis.
An observational study found that adjuvant chemotherapy improves overall survival in patients with locally advanced bladder cancer.
Despite a high rate of hematologic toxicity, combined low-dose gemcitabine (Gemzar), paclitaxel, and sorafenib (Nexavar) showed promise as a well-tolerated salvage therapy in a small group of patients with cisplatin-resistant urothelial cancer.
An Egyptian study found that bladder cancer patients who underwent radical cystectomy had better local recurrence-free survival with adjuvant radiotherapy and chemotherapy combined, compared with chemotherapy alone.
The anti-PD-L1 antibody atezolizumab showed significantly improved objective response rates compared to historic controls in a phase II study of patients with locally advanced or metastatic urothelial carcinoma previously treated with platinum-based therapy.
Comprehensive genomic profiling of patients with advanced urothelial carcinoma has revealed a very high frequency of clinically relevant genomic alterations.
Patients with metastatic or unresectable urothelial carcinoma who are treated with either carboplatin or cisplatin have high rates of vascular thromboembolic events.
A phase II trial found that use of a personalized peptide vaccination improved overall survival in patients with chemotherapy-resistant advanced urothelial bladder cancer.
In most cases, localized small-cell bladder cancer requires cystectomy for optimal cure rates.
Radiation therapy with concurrent chemotherapy is an effective treatment strategy for small-cell bladder cancer.
Use of the diabetes drug pioglitazone was not associated with a significantly increased risk of bladder cancer, in a large cohort study.
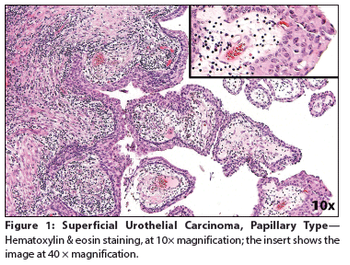
A 65-year-old woman presented to a local emergency department complaining of right flank pain that had worsened over the past 10 days. A CT scan of the abdomen and pelvis showed intravesical tumors of the urinary bladder.
Pembrolizumab demonstrates durable antitumor activity in patients with advanced urothelial cancer, with a higher response rate seen in patients with PD-L1 expression.
Advanced bladder cancer patients with poor prognosis appear to benefit from adding apatorsen 600 mg to first-line chemotherapy with gemcitabine/cisplatin.
Advertisement
Advertisement
Trending on CancerNetwork
1
Study Redefines Functional High-Risk Multiple Myeloma in Modern-Therapy Era
2
ctDNA MRD Guidance in Bladder Cancer: Pharmacy Specialist on NCCN Updates
3
Sequencing Treatment after EV-Pembro in Urothelial Carcinoma
4
Managing Safety and Infection Risk With Bispecific Antibodies in Relapsed/Refractory Multiple Myeloma
5