The question of a well-defined role for the use of neoadjuvant chemotherapy in the treatment of ovarian cancer is recognized to be one of the most hotly debated issues in the management of female pelvic malignancies.[1-3] One group of oncologists would argue that it should be the rare patient (eg, with severe comorbidity) who is not a candidate for an initial attempt at maximal cytoreduction.[1]
ONCOLOGY Vol 22 No 10
Ovarian cancer is a unique malignancy. While the disease can spread hematogenously or via the lymphatic system, the bulk of the tumor is found on peritoneal surfaces. This peritoneal disease results from shedding of ovarian tumor cells into the peritoneal cavity, circulation of these cells throughout the abdomen and pelvis, and eventual implantation onto peritoneal surfaces.
Conventional therapy for advanced-stage ovarian cancer-ie, aggressive cytoreductive surgery followed by aggressive chemotherapy-was established more than 3 decades ago [Editor’s note: See Dr. Schwartz’s article, “Cytoreductive Surgery in the Management of Ovarian Cancer,” in last month’s issue of ONCOLOGY]. Since that time, no prospective randomized trials have been reported to confirm the efficacy of this treatment strategy.
Primary carcinoma of the vagina accounts for 1% to 3% of all gynecologic malignancies, with 70% of cases occurring in women over age 60.[1] Hematogenous dissemination is rare at diagnosis but is more common in patients with advanced, neglected lesions.
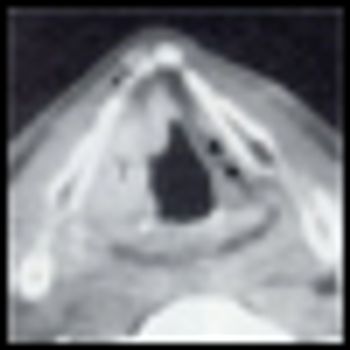
About 500,000 head and neck carcinomas are diagnosed worldwide annually. This accounts for approximately 8% of all newly diagnosed cases of cancer, ranking head and neck carcinoma the sixth most common.[1] In the United States, 47,560 new head and neck carcinomas are expected to be diagnosed in 2008,[2] and this disease accounts for 5% of all newly diagnosed cases of cancer. Approximately 90% to 95% are squamous cell carcinomas of the head and neck (SCCHNs).
Gemcitabine (Gemzar)-based regimens have been the mainstay of front-line treatment for patients who present with advanced pancreatic cancer over the past decade, but most medical oncologists throw their hands up in frustration when considering what therapeutic options a patient is left with once he or she has progressed beyond first-line therapy. This is not without reason-as nicely summarized in the review article by Almhanna and Kim, studies in the published medical literature focusing on treatment of pancreatic cancer in the salvage setting have generally been small and have shown very modest clinical efficacy, characterized by low response rates and progression-free survival of a few months at best.
Vaginal carcinoma is rare, accounting for 1% to 2% of female genital cancers.[1] Squamous cell cancer accounts for 80% to 90% of vaginal cancers. Human papillomavirus (HPV) viral particles can be identified in approximately 60% of invasive squamous cancers of the vagina.[2]
In the past, locoregionally advanced head and neck cancer routinely was treated by surgery followed by adjuvant radiation therapy, unless the disease was too extensive to be resected and treatment defaulted to radiation therapy alone.
Bruce Culliney and colleagues have provided a thorough and well written summary of the literature regarding multimodality treatment of patients with locoregionally advanced or unresectable head and neck malignancies. In particular, they offer a detailed outline of recent insights into radiation dosing and fractionation and their optimal use in the combined-modality setting.
In this first installment of ONCOLOGY’s new department, we review “graviola.” Graviola was chosen for review because it is one of the most commonly searched terms sought by visitors to MSKCC’s “About Herbs” website. Because graviola is commonly promoted as a cancer treatment, your patients may be inclined to take it.
The US Food and Drug Administration (FDA) has approved a new oral formulation of palonosetron hydrochloride (Aloxi) for the prevention of chemotherapy-induced nausea and vomiting (CINV). Oral administration of palonosetron capsules is indicated for the prevention of acute nausea and vomiting following initial and repeat courses of moderately emetogenic chemotherapy. A single 0.5-mg palonosetron capsule is administered approximately 1 hour prior to the start of chemotherapy.
Patients with advanced renal cell carcinoma (RCC) treated with single-agent, oral sunitinib malate (Sutent) reported experiencing significantly lower severity of symptoms like bone pain and breathlessness, among others, than patients treated with interferon-alfa.
Factors such as age at menopause and a woman’s breast-feeding practices can influence her risk of developing certain types of breast cancer. That was the conclusion of a new study to be published in the October 1, 2008, issue of CANCER. The study’s results suggest that there are distinct and separate hormonal risk factors associated with different subtypes of breast cancer.
In the following sections, we will first review the radiotherapy techniques that have been investigated. We will then review the progressive advances achieved with the addition of chemotherapeutic strategies to RT in an attempt to achieve better outcomes.
Pancreatic cancer is the fourth leading cause of cancer mortality in the United States. According the American Cancer Society, about 37,680 new cases are anticipated in the year 2008, and 34,290 patients will die from the disease.[1] This malignancy is a very aggressive tumor, and patients often present with advanced-stage disease. Surgical resection, when possible, provides the only opportunity for cure. Even with R0 resection, pancreatic cancer still carries an overall dismal prognosis, and therefore adjuvant treatment is offered.
The paper by Almhanna and Kim addresses a clinical dilemma in the treatment of pancreatic cancer, for which no standard currently exists. The review article concisely summarizes studies in the second-line setting that have been conducted to date, many of which have been published only in abstract form. The authors organize the studies into tables according to the number of agents in the trials and highlight the response rates and toxicities. The inclusion of study endpoints (both primary and secondary) would have made the tables more informative. In the article, the studies are organized according to the specific agent studied. Several of the studies continue to use gemcitabine (Gemzar) in combination with other agents in the second-line setting, but we have insufficient data to determine that continuing gemcitabine in this setting is worthwhile.
Advertisement
Advertisement
Trending on CancerNetwork
1
FDA Accepts NDA for Mezigdomide Combo in R/R Multiple Myeloma
2
Dostarlimab Yields Sustained Complete Responses in dMMR/MSI-H Rectal Cancer
3
Risvutatug Rezetecan Improves Overall Survival in Relapsed SCLC Trial
4
ADCs in the Frontline: Evolving Approaches in Metastatic TNBC
5