
This study adds to the evidence that the decline in access to local care due to the shuttering of rural hospitals and community cancer clinics adversely affects cancer patients.
This study adds to the evidence that the decline in access to local care due to the shuttering of rural hospitals and community cancer clinics adversely affects cancer patients.

The FDA approved selinexor in combination with the corticosteroid dexamethasone for the treatment of adult patients with relapsed/refractory multiple myeloma.

Healthy eating, exercise, and avoiding smoking can save lives. So why aren't more doctors talking to patients about lifestyle changes?
The FDA approved daratumumab in combination with lenalidomide and dexamethasone for patients with newly diagnosed multiple myeloma who are ineligible for autologous stem cell transplant.

A new trial investigated the efficacy of XELOX vs GEMOX as first-line therapy for advanced biliary tract cancers.

Many patients complain of "chemo brain," or a drop in cognitive function during or after receiving chemotherapy, but there are strategies to manage chemo brain, as well as research on how chemotherapy affects the brain long-term.

This article reviews the prevalence of suicide in patients with cancer, risk factors, related conditions, and interventions to identify and treat suicidal patients.
The FDA approved pembrolizumab as a treatment option for patients with metastatic small-cell lung cancer.
The FDA approved pembrolizumab for the first-line treatment of patients with metastatic or unresectable recurrent head and neck squamous cell carcinoma.
The FDA granted accelerated approval to polatuzumab vedotin-piiq, a CD79b-directed antibody-drug conjugate, in combination with bendamustine and a rituximab product for adult patients with relapsed or refractory diffuse large B-cell lymphoma.
In this video, Dr. McFarland of Memorial Sloan-Kettering Cancer Center spoke with Cancer Network at ASCO 2019 about depression in lung cancer and dopamine as potential therapy.

Researchers are reporting that previous racial disparities in timely cancer treatment between African American and white patients practically disappeared in states where Medicaid access was expanded under the ACA.

This slideshow reviews the latest clinical updates surrounding the management of treatment-associated nausea and vomiting, including recommendations, newly approved agents, and more.

A worldwide crowd innovation contest incentivized international programmers to create automated AI algorithms for an area of radiation oncology.

The findings further validate the initial 2015 findings that a five-fraction SBRT schedule is appropriate for patients with centrally located NSCLC.
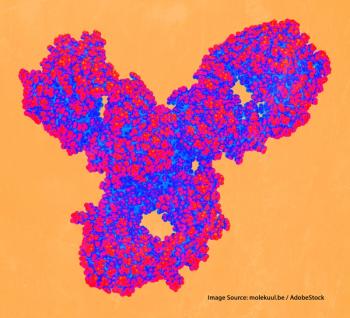
The percentage of patients with cancer eligible to receive immune checkpoint inhibitors has increased in recent years, but how many patients are actually responding?

Cancer Network spoke with Dr. Scarlett Lin Gomez about the role gender, socioeconomic status, race/ethnicity, and neighborhood characteristics have on health outcomes in cancer.
The investigators tested the agent in patients who had solid tumors with NTRK gene fusions that had developed resistance to other TRK inhibitors.
A phase I trial evaluated the safety and efficacy of adding lymphodepletion to HER2-targeted T-cell therapy in patients with advanced HER2-positive sarcoma.
This slideshow summarizes recent US Food and Drug Administration approvals of new oncology drugs and oncology drug indications.

Researchers looked at the trends and risk factors for opioid-related hospitalizations among patients with cancer.

A series of communication-focused interventions were implemented to try to improve conversations about values, goals, and preferences with patients with life-limiting cancer.

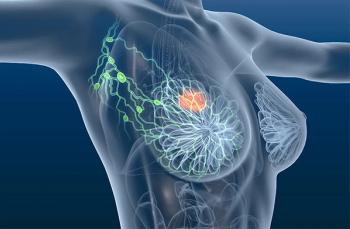
Cancer Network spoke with Charles Shapiro, MD, about the USPSTF's stance on use of tamoxifen, raloxifene, and aromatase inhibitors to prevent breast cancer.

A single-center evaluation of the FDA's Expanded Access program indicated broad use of the program among the center’s patients, including a large percentage of pediatric patients.
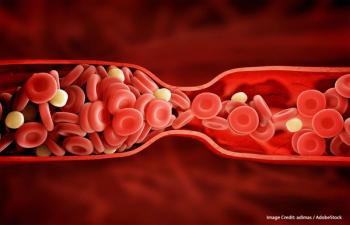
In a phase IIIb trial, researchers evaluated the efficacy of an oral anticoagulant in cancer patients at high risk for venous thromboembolism.
A systematic review in JAMA Oncology examined the safety and efficacy of immune checkpoint inhibitors in advanced-stage cancer patients with HIV infection.

The US Food and Drug Administration explored the possibility of such bias in a recent viewpoint published in JAMA Oncology.

Cancer Network speaks with Joseph Unger, PhD, about ways to decrease the barriers for cancer patients to enroll in clinical trials.

Cancer Network speaks with an exercise physiologist about the benefits of physical activity for depressed and anxious cancer patients.

Do race, income level, geographic location, and type of specialist influence treatment of metastatic castration-resistant prostate cancer?