
Many trials in the last decade that have led to FDA drug approvals didn't report on race and the ones that did were lacking in racial diversity.
Many trials in the last decade that have led to FDA drug approvals didn't report on race and the ones that did were lacking in racial diversity.
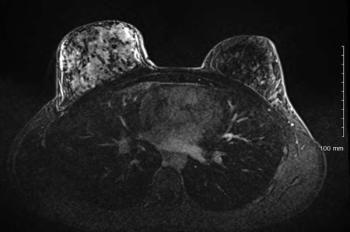
A 22-year-old Caucasian woman presents with a four month history of pain, tenderness and swelling in her right breast. What's your diagnosis?
A new study looked at what methods were used to detect recurrences of human papillomavirus (HPV)-associated oropharyngeal squamous cell carcinoma to see if surveillance guidelines recommended by the National Comprehensive Cancer Center were effective.

Laparoscopic treatment during pregnancy is becoming an option for more women.


Cancer Network spoke with Kelly Hunt, MD, professor and chair of the department of breast surgical oncology at the MD Anderson Cancer Center in Houston, about the role of surgery in metastatic breast cancer.
There are continued advances in the use of biomarkers to guide drug development and the more targeted delivery of medicine.

The U.S. Preventive Services Task Force released a new review of the benefits and harms of imaging-based screening for pancreatic cancer.

Despite the toll chemotherapy can take on the body, experts say it's possible for athletes to exercise while undergoing treatment for cancer.


Researchers looked at data from the Surveillance, Epidemiology, and End Results database to see if there has been any increase in the use of active surveillance or watchful waiting when it comes to low-risk prostate cancer.

How much do you know about the epidemiology and prognosis of ovarian cancer? Here's your chance to find out.
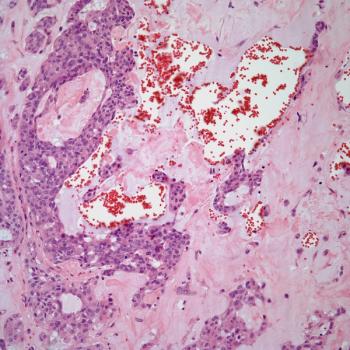
A 41-year-old woman presents with a palpable mass in her left breast. A lumpectomy is performed. What is your diagnosis?

In 2017, about half of physician directors at National Cancer Institute cancer centers received payments related to research, while a quarter received payments over $5,000 that were not related to research.
The United States Preventive Services Task Force issued a statement reaffirming its 2004 recommendation against screening for pancreatic cancer in asymptomatic adults.

A phase III trial found bevacizumab and pemetrexed were effective as a maintenance therapy, but researchers do not recommend it to treat non–small-cell lung cancer.

Researchers tried using deep machine learning to anticipate disease outcomes and progression in patients with lung cancer.

The phase II study compared single-agent anti-EGFR panitumumab to panitumumab combined with fluorouracil-leucovorin in patients with RAS wild-type metastatic colorectal cancer.

Researchers examined the rate and risk of late-onset anorectal disease among childhood cancer survivors.
Researchers looked at diagnosis, assessment, treatment, and prognosis of women diagnosed with cervical cancer while pregnant.

This new study looked at chronic pain rates among cancer survivors, including which survivors report the highest prevalence of pain.

A survey of oncologists found child care is a significant concern of women in the field and can greatly impact their conference attendance compared to their male counterparts.
A new study offers hope in predicting glioblastoma responses to chemotherapy, radiation, and combination therapy.
The risk of multiple primary cancers is increasing due to increasing numbers of survivors, long-term side effects of chemotherapy and/or radiation therapy, increased diagnostic sensitivity, and persisting effects of genetic and behavioral risk factors.
Researchers looked at whether or not a two-dose recombinant zoster vaccine would reduce the incidence of herpes zoster in patients with hematologic malignancies after autologous stem cell transplantation.

A new study estimated that cancer deaths in 2015 resulted in billions in lost earnings in the United States.