
Cancer Network speaks with Dr. Leon Ptaszek about managing cancer patients who have atrial fibrillation and are being treated with BTK inhibitors.
Cancer Network speaks with Dr. Leon Ptaszek about managing cancer patients who have atrial fibrillation and are being treated with BTK inhibitors.

Survey results published in JAMA Network Open looked at motivating factors behind patient travel and how far they were willing to go for treatment.

Gary H. Lyman, MD, MPH, says the plan does not address several significant concerns, such as delay tactics that limit prompt access to biosimilars.

Guy Ben-Betzalel, MD spoke with Cancer Network about the emerging role of targeted BRAF+MEK inhibition in antitumor immunity.

Professor Lana E. Kandalaft, PharmD, PhD spoke with Cancer Network about the next generation of cancer immunotherapy.

A recent study in JAMA Oncology examined the average daily cost of biosimilar filgrastim-sndz compared with the brand name biologic.

Stephanie Jackson, MSN, RN speaks with Cancer Network about the role oncology nurses play in managing patients with hematologic malignancies who are undergoing CAR T-cell therapy.

This article discusses some of the popular diets that cancer patients pursue, and the positive and negative aspects associated with these diets.

A study in Thyroid evaluated the safety and efficacy of concurrent intensity-modulated radiation therapy and doxorubicin in thyroid cancer.

We spoke with Erin McMenamin, CRNP, of Penn Medicine, about the recent study on opioid switching in cancer patients.

Interim results are in from a study evaluating whether adding selumetinib to RAI improves complete response, irrespective of MAPK pathway alterations.

We spoke with Kelly Hogan, MS, RD, about the recent JAMA study on the association between organic food consumption and cancer risk.

The findings of this study, recently published in JAMA Oncology, directly contradict previously conducted research on the same topic.
Oncologists now have some clarification on the use of moderate hypofractionation and ultrahypofractionation from ASTRO, ASCO, and the AUA.

Dr. Denise Faustman spoke with Cancer Network about TNFR2 and its emerging role in understanding regulatory T-cell behavior.

Dr. William Newman spoke with Cancer Network about the roles of epigenetic silencing in heritable cancer syndromes.

A study of more than 350 hospitals found variations in readmission and mortality rates after cancer surgical procedures.

Various challenges still surround the use of cancer biologics, but expert guidance and expiring patents may help expand their use and benefits.

Dr. William Pirl speaks with Cancer Network about cancer patients' moods influencing their well-being and survival.
Research presented this week at ESMO studied the efficacy of biosimilars to trastuzumab compared with the reference product in breast cancer.
A new study evaluated whether busulfan and melphalan improve EFS and OS when given after vincristine, ifosfamide, doxorubicin, and etoposide induction.
Professor Han Liang speaks with Cancer Network about the ubiquitin pathway and its role in cancer research.
Guang Peng, MD, PhD spoke to Cancer Network about the recent discovery that mTORC1 can help determine cell fate after DNA damage.

Dr. Raghu Kalluri speaks with Cancer Network about the role of exosomes in cancer progression ahead of his presentation at ESMO 2018.

In his latest blog, Craig Hildreth explores the terror of the black box warning and how the fear of toxicities affects his patients-and his staff.

Dr. Ian Flinn spoke with Cancer Network about incorporating the newest approved therapies for the management of CLL.

In this article, we describe the mechanisms via which interactions between herbs and prescription drugs may occur, and highlight four popular herbs and a medicinal mushroom commonly used by cancer patients, along with reports of their interactions with standard drugs.

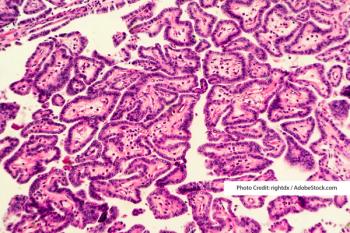
A new study in Cancer Management and Research found a correlation between the age of patients with papillary thyroid cancer and lymph node positivity.
LOXO-292, which selectively targets RET and has demonstrated preclinical activity against activating RET fusions/mutations, holds promise.