
We take a look at how a healthy diet can improve quality of life in breast cancer survivors.
We take a look at how a healthy diet can improve quality of life in breast cancer survivors.
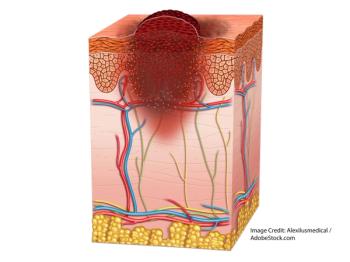
Cemiplimab (Libtayo), approved for advanced cutaneous squamous cell carcinoma, is intended for those not eligible for curative surgery or radiation.
Cervical cancer is the most common HPV-associated cancer. What are some of the others? Take our quiz to test your knowledge.

Dianne Shumay, PhD, director of psycho-oncology at UCSF, weighs in on how we can use psychological interventions to improve stress levels in cancer patients.
A study shows gene variants of uncertain significance are frequently reclassified, necessitating amended test result reports.

The FDA authorized the first next-generation sequencing test to detect minimal residual disease in blood cancers.

Patients with von Hippel-Lindau disease may have a new treatment option in the antiangiogenic therapy pazopanib.

Nanotechnological strategies are making preclinical strides toward more effective, less toxic, immunotherapies.
A study shows TRK gene fusions in hematologic cancers may respond to larotrectinib.

The eighth edition outperforms the seventh edition in predicting survival differences in patients with papillary thyroid cancer and follicular thyroid cancer.
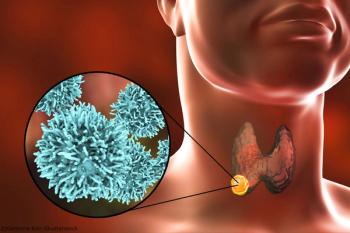
The study confirmed a significant effect of male sex on PTC-specific patient survival in individuals with the most frequent oncogenic mutation.

Professor Judi Fouladbakhsh speaks with Cancer Network about evidence-based holistic approaches to cancer care.
Certain malignancies may possess a common and targetable matrix response, which affects disease pathogeneis, according to a study in Cancer Discovery.
Dr. Dmitriy Zamarin speaks with Cancer Network about the findings of a phase II trial in platinum-resistant ovarian cancer patients.

Individuals who develop frequent basal cell carcinomas may have an increased prevalence of germline mutations in DNA repair genes and an increased malignancy risk.
New research examines the mechanisms underlying why most patients with high-grade serous ovarian cancer develop resistance to PARP inhibitors.

Linda Jacobs, PhD, CRNP, director of the Cancer Survivorship Center, comments on the incidence of erectile dysfunction in childhood cancer survivors.

Researchers have developed a mouse model of high-grade serous carcinoma that could prove useful in the preclinical testing of prevention strategies for ovarian cancer.

Optical coherence tomography and multispectral fluorescence imaging have demonstrated promising results in the early detection of ovarian cancer.

Breast and gynecologic cancer patients undergoing chemotherapy may experience improvement in cancer-related fatigue with integrative medicine approaches.

Dr. Ranjit Manchanda speaks with Cancer Network about using population testing to predict and prevent gynecologic cancers.
A particular gatekeeper-the nuclear pore protein called POM121-traffics molecules that increase tumor aggressiveness in prostate cancer.

A study finds EWSR1-ETS in 42% of cases via complex, loop-like rearrangements, rather than by simple reciprocal translocations.

Mogamulizumab (Poteligeo) is indicated for relapsed or refractory mycosis fungoides or Sézary syndrome following at least one prior systemic therapy.
A study shows significant association between MTHFR C677T polymorphisms and risk of oral squamous cell carcinoma.

The number of nurse practitioners and physician assistants in oncology is growing, according to a new study.
The guidelines will better ensure pregnant cancer patients receive life-saving treatment while preserving fertility.

For patients undergoing primary treatment for head and neck cancer, sexuality was significantly impacted in many patients both prior to and during cancer treatment.

VOC breath tests have potential, but more guidance, standardization are needed.

A retrospective study shows that undergoing oral care prior to cancer surgery decreased postoperative complications.