Experience with the recently enacted California End of Life Option Act has shown that a high percentage of patients who requested aid-in-dying drugs in California have proceeded with ingesting the drugs. The majority of these requests were made by terminal cancer patients.
All News
Survival disparities for black patients with ovarian, colon, and breast cancer and childhood ALL suggest a need for efforts toward improved screening and treatment adherence in this population.
Advertisement

In this interview, we discuss a mathematical model that was created to predict patient response to immunotherapy for cancer treatment.
A recent analysis from the Breast Cancer Surveillance Consortium revealed that community oncology practices are neglecting to use MRI screening for at-risk women, and lower-risk women are being unnecessarily screened.
Advertisement
A new study has found that there are significant gaps in participation among people aged 75 and older in clinical trials of hematologic malignancies when considered against the incidence of these malignancies in this age group.
The needs and challenges of cancer survivors and their family members do not vanish once treatment has been completed, although their follow-up care is often not addressed sufficiently.
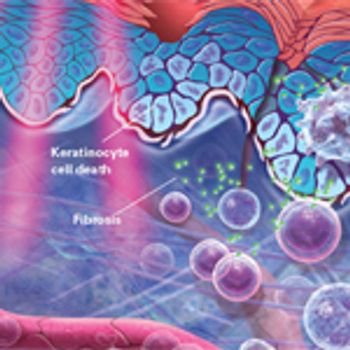
This article highlights the typical skin reactions associated with RT, as well as current evidence-based approaches to management and intervention.

In this interview we discuss the goals of SIO, the response to donations intended for interdisciplinary integrative health, and how palliative care and psychosocial oncology can enhance each other.
Patients with gastrointestinal neuroendocrine tumors with carcinoid syndrome are more than twice as likely to have certain pre-existing diagnoses compared with patients without carcinoid syndrome, according to the results of a study.
Patient access to NCI Cancer Centers is influenced by a complex mix of cancer center distribution and density, ethnicity, urbanicity, and travel time to care, according to a recently published statistical model.
Post-traumatic stress disorder may be persistent or worsening in patients with cancer up to 4 years after an initial diagnosis of the disorder, according to the results of a study.
Rolapitant plus 5-HT3 receptor antagonist and dexamethasone is well tolerated and more effectively controls chemotherapy-induced nausea and vomiting compared with 5-HT3 and dexamethasone alone.
Researchers found that combining palonosetron, aprepitant, and dexamethasone represents an effective and well-tolerated treatment to prevent CINV in testicular cancer patients receiving cisplatin.
A recent study showed that molecular tumor boards coupled with cognitive computing with IBM's Watson could improve patient care by providing a rapid, comprehensive approach for data analysis.
A novel classification system that incorporates genomic risk with clinical variables was able to accurately identify prostate cancer patients at low, intermediate, and high risk for metastasis.

The FDA approved a biosimilar for trastuzumab, Ogivri, for the treatment of patients with HER2-positive breast and stomach cancer.
More than half of young adult cancer patients reported ongoing problems related to sexual function during the first 2 years after their cancer diagnosis.
Mood disorders are common mental health sequelae of cancer, but depression in patients with cancer is frequently missed by healthcare providers, and there are many reasons for this oversight.

It is an exciting time for science, but lest we forget, those of us who provide direct patient care are also charged with practicing the art of medicine.

This video reviews the benefits of proton therapy and some of the barriers and challenges preventing the integration of the technology into regular practice.
Aprepitant plus palonosetron and dexamethasone showed early promise for preventing chemotherapy-induced nausea and vomiting among patients with colorectal cancer who are undergoing FOLFOX chemotherapy, according to results of a small pilot study.
Combined analysis of risk factors predicts long-term cardiovascular complications in childhood cancer survivors more accurately than single-factor assessments.

This slide show highlights some of this year’s FDA approvals of cancer treatments, including new therapies and indications for breast cancer, lung cancer, and various blood cancers, as well as the first approval based not on disease site but by tumor marker.

A precision medicine clinical trial based on genomic abnormalities has screened nearly 6,000 patients in just under 2 years and matched 18% of tumors screened with a genetic mutation to one of 30 treatment arms.
Men with Medicaid are more likely to present with metastatic prostate cancer than men presenting with prostate cancer who have private insurance, according to a new study. There are racial disparities in terms of prostate cancer outcomes among those privately insured, but not among Medicaid recipients.
The FDA has approved rolapitant injectable emulsion in combination with other antiemetics in adults to prevent delayed chemotherapy-induced nausea and vomiting.
The Commission on Future Research Priorities in the USA sets out 13 key priority areas to help focus the $2 billion of funding released to the NCI.

This slide show highlights some of the studies and analyses that have explored physical activity/exercise and its effect on cancer risk, as well as studies that examined physical activity and its effect on treatment side effects from chemotherapy, radiotherapy, and surgery.
Advertisement
Advertisement
Trending on CancerNetwork
1
Epcoritamab Combo Shows Sustained Remissions in Follicular Lymphoma
2
Olomorasib Earns FDA Breakthrough Therapy in KRAS G12C+ Pancreatic Cancer
3
GLP-1 Receptor Agonists and Cancer: Renewed Momentum for Metabo-Oncology
4
Understanding The Training, Credentialing Landscapes for End-of-Life Doulas
5