In a study of over 100,000 adults, overall cancer risk, particularly of breast cancer, was associated with dietary intake of ultra-processed foods.
All News
Earlier collection of patient-reported outcomes could potentially improve comprehensive cancer care.
Advertisement

A review of the rules of the road for doctors, because everyone remembers their first license.
The significant tumor shrinkage and immunologic changes observed support a complementary role of SBRT and PD-1 immunotherapy, investigators concluded.
Early-phase data on larotrectinib validate TRK fusions as therapeutic targets and show they lead to tumor-agnostic sensitivity to this agent.
An early phase trial found that it is feasible to combine nivolumab immunotherapy with radiation therapy and chemotherapy in patients with newly diagnosed local-regionally advanced head and neck cancers.
Advertisement
Patients with human papillomavirus–associated head and neck cancers who respond well to induction therapy can receive substantially lower doses of radiation and still achieve good safety and efficacy outcomes, according to a new phase II trial.
Patients with familial adenomatous polyposis have an increased risk for colorectal polyps and cancer; however, treatment with a combination of sulindac and erlotinib reduced their colorectal polyp burden by more than two thirds.

Coffee may soon contain a warning that it contains acrylamide, a known carcinogen. A recent lawsuit filed by the nonprofit Council for Education and Research in Toxics alleges that coffee shops in California “failed to provide clear and reasonable warning” that their product could expose people to acrylamide.

Typical cell phone use is unlikely to cause cancer via radiation exposure, according to government researchers.
A class of small molecules called parmodulins may be able to reduce inflammation without compromising normal blood clotting, making them attractive candidates for new, safer drugs.
A new multianalyte test simultaneously evaluates levels of eight cancer proteins and the presence of cancer gene mutations from circulating DNA in the blood, offering clinicians and patients a potentially affordable way of detecting cancer at an earlier stage.
A new study has revealed that the amount of iron in the blood affects the amount of the Scribble protein, which appears to control receptors that create new red blood cells.

Last year saw the first two FDA approvals of oncology biosimilars, but experts have voiced concerns about the emerging US biosimilars market, particularly regarding clinical uptake and uncertainty about costs.

In this slide show we highlight some of the top news from the past year on genetic testing for cancer, including gene signatures for identifying different sub-types of breast cancer, the influence of genetics on RCC outcomes, and the utility of liquid biopsies.
Adjuvant radiotherapy after prostatectomy resulted in lower rates of biochemical recurrence, distant metastases, and death compared with surveillance followed by early-salvage radiotherapy in patients with high-risk prostate cancer, according to a new study.
The largest and most up-to-date study of international cancer registries shows that survival trends are generally increasing, even for some lethal cancers.

The US Food and Drug Administration approved lutetium Lu 177 dotatate (Lutathera) for the treatment of somatostatin receptor–positive gastroenteropancreatic neuroendocrine tumors in adults.
Investigators found a methylation-independent loss of MYO5B expression in CRC that matched disease progression, which indicates that the use of MYO5B alone or in combination with its adapter protein RAB8A is a prognostic marker for the disease.
Using a super computer, a team at Brown University has created a model of sickle cell anemia, devising a method that could help researchers assess and evaluate treatments to combat sickle cell disease.
ASCO recently released a clinical practice guideline on the treatment of malignant pleural mesothelioma, including recommendations on diagnosis, staging, and treatment with chemotherapy, surgical cytoreduction, and radiation therapy.
Using gene expression profile tests like Oncotype DX to inform treatment decision-making for breast cancer is likely to be less cost-effective in community oncology practice than previous estimates had suggested.
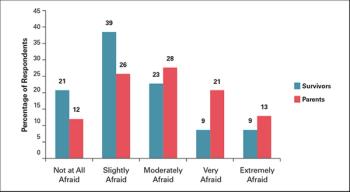
Here, we review the barriers to adherence, including those unique to childhood cancer survivors, and the rationale for distribution of a survivorship care plan. We also discuss advantages and potential limitations of delivering survivorship care plans via web-based platforms, and describe the unique features of one of these platforms, Passport for Care.
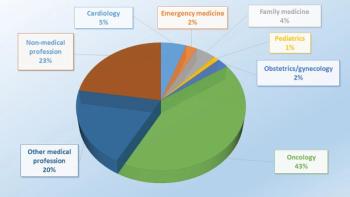
Last month we asked our readers: If you were to start your career again, would you still choose oncology, would you pick a different specialty, or would you perhaps not choose a career in medicine at all? Here are the results.

This video reviews endocrine resistance mediated by CDK4/6, FGFR, and PI3K in HR-positive breast cancer, and highlights the latest efforts to inhibit these pathways with novel targeted drugs and combinations.

Learn about what motivational pharmacology is and is not in this quiz.

This video highlights a study on optoacoustic imaging, a new type of imaging that could improve breast cancer diagnosis by differentiating between benign and malignant breast masses.
A new study has shown several ways that the health-related quality of life in cancer patients older than 65 years could be improved.
Advertisement
Advertisement
Trending on CancerNetwork
1
Epcoritamab Combo Shows Sustained Remissions in Follicular Lymphoma
2
Olomorasib Earns FDA Breakthrough Therapy in KRAS G12C+ Pancreatic Cancer
3
GLP-1 Receptor Agonists and Cancer: Renewed Momentum for Metabo-Oncology
4
Understanding The Training, Credentialing Landscapes for End-of-Life Doulas
5