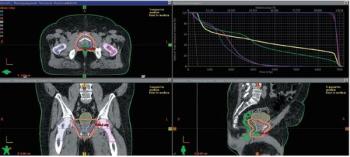
A 62-year-old man with prostate adenocarcinoma elected to proceed with radical prostatectomy as definitive management. After his pathology report showed stage IIIB disease, he elected for observation. What happened next?
A 62-year-old man with prostate adenocarcinoma elected to proceed with radical prostatectomy as definitive management. After his pathology report showed stage IIIB disease, he elected for observation. What happened next?
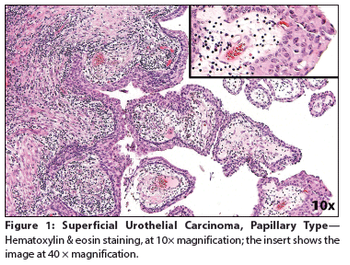
A 70-year-old man presented at our institution for a second opinion regarding diagnosis of a urinary bladder mass. He had a 3-year history of worsening urinary incontinence and urgency, for which he had undergone colonoscopy, as well as testing for prostate issues; all test results were negative.
A 65-year-old woman presented to a local emergency department complaining of right flank pain that had worsened over the past 10 days. A CT scan of the abdomen and pelvis showed intravesical tumors of the urinary bladder.
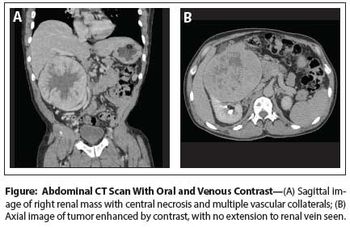
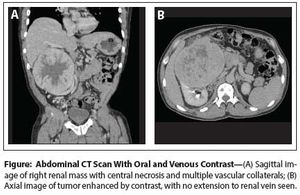
Case History: 60-year-old man with mild right side abdominal discomfort and hepatomegaly found to have large right renal mass during CT scan.
As long as there is any risk of progression, G6 cancer cannot be equated to just a precursor lesion, and the emphasis should remain on screening patients with serum PSA measurement, contrary to the recommendation of the US Preventive Services Task Force.
The patient is a 66-year-old male who presented to his primary care physician with a 3-week history of painless gross hematuria. He underwent a renal ultrasound that showed a left kidney mass.
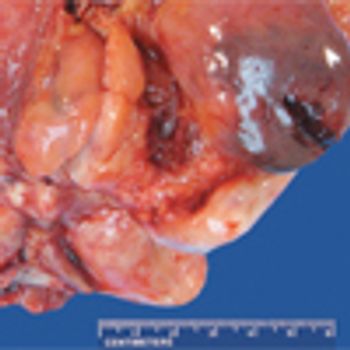
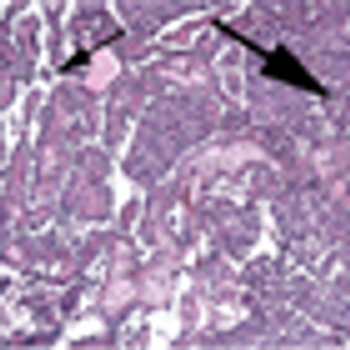
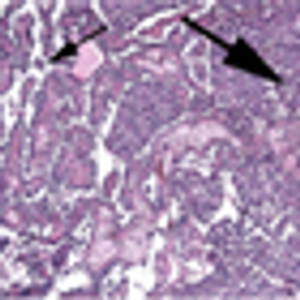
The patient is a 43-year-old man who was initially evaluated at an outside institution for unexplained anemia and who was found to have a large right kidney mass. He underwent a radical nephrectomy for a 19-cm large-cell, poorly differentiated neoplasm, consistent with pleomorphic, epithelioid angiomyolipoma (EAML) with extensive necrosis and cytologic atypia.

The patient is a 26-year-old woman with a complex oncologic history. At 1 year of age, she was diagnosed with a stage III abdominal neuroblastoma, which was treated, and again at age 9, she had a recurrence of neuroblastoma in the left axilla. She was in her usual state of good health until 18 months ago, when she presented with hematuria and was found to have a right-sided kidney mass.
A 56-year-old woman was referred to our institution for a left nephroureterectomy after the diagnoses of a nonfunctioning left kidney and noninvasive papillary urothelial carcinoma of the distal left ureter (Ta grade 1). Following the procedure, surveillance cystoscopy and computed tomography (CT) scan of the abdomen and pelvis demonstrated a large bladder tumor with pan-urothelial extension.

The patient is a 39-year-old man who presents with pelvic lymphadenopathy. He has a history of ureteral reflux disease, recurrent nephrolithiasis, right nephrectomy, ileal loop diversion of the left ureter, and radical cystectomy for “bladder cancer,” which he underwent 3 years ago. The lymphadenopathy was discovered incidentally during recent imaging.
The patient is a 39-year-old Caucasian male who presented with a right renal mass and painless gross hematuria. He underwent a right laparoscopic radical nephrectomy and the final pathology revealed a carcinoid tumor.
patient is a 67-year-old male with mild obstructive symptoms and an American Urology Association symptom score of 8.[1] He was noted to have a prostate-specific antigen (PSA) level of 3.2 ng/mL. Because this represented a significant increase in his PSA velocity (rate of change over time), he proceeded to have a biopsy, which was positive for prostate cancer. He has no other complaints and visits us for an opinion on the treatment of his prostate cancer.

March 22nd 2010
January 15th 2014
September 15th 2013
April 15th 2014
December 16th 2009
