
Should I give a patient with a carcinoma of unknown primary another dose of a study drug, since she is requesting to continue it? My reading of the trial protocol suggests no absolute restriction on giving another dose of the drug.
Should I give a patient with a carcinoma of unknown primary another dose of a study drug, since she is requesting to continue it? My reading of the trial protocol suggests no absolute restriction on giving another dose of the drug.
Bladder neoplasms are associated with a high frequency of painless hematuria; however, when compared with the bleeding tendencies of other solid tumors, it is arguable that this comparatively high bleeding frequency is in part the result of an ascertainment bias.
Overall, approximately 2% of patients with bladder cancer will experience a venous thromboembolism event, a rate five times higher than that in the overall population; also, such an event results in a threefold increased risk of death in patients with cancer.
Cancer promotes the development of venous thromboembolism (VTE) by inducing a hypercoaguable state, through mechanisms that are complex and multifactorial.
Despite the higher risk of VTE in patients with bladder cancer, ironically, their risk of bleeding and anemia, and greater need for transfusion of blood products, poses an equally significant risk of morbidity and mortality, especially among those who undergo cystectomy.

Ultimately, while further follow-up will be enlightening, we believe that there is sufficient evidence now from the primary analysis of CHAARTED to justify the combination of docetaxel and androgen deprivation therapy in all men with metastatic hormone-sensitive prostate cancer.

Meta-analyses of patients with low-volume metastatic hormone-sensitive prostate cancer will likely be required to attain sufficient power to address the role of docetaxel in this setting.
Treatment-emergent small-cell/neuroendocrine prostate cancer is likely to become of increasing clinical relevance in the era of widespread use of potent androgen receptor–targeted therapies.
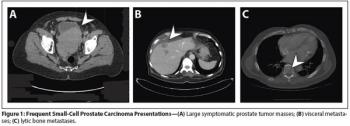
Aggressive variants of prostate cancer often take the form of neuroendocrine or small-cell carcinomas, which frequently lack androgen receptor expression and respond poorly to hormonal therapies.
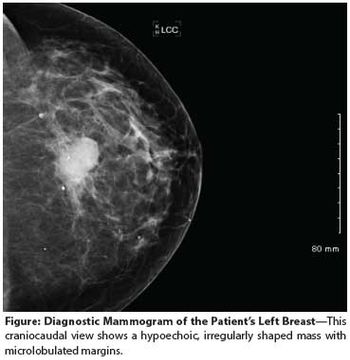
A 24-year-old woman presents to her primary care provider with a mass in her left breast. Examination confirms a 2.2-cm mass in the upper outer quadrant, with a single mobile axillary node that is firm to palpation.