



















































































The myelodysplastic syndromes (MDS) are a heterogeneous spectrum of clonal hematopoietic diseases characterized by bone marrow hypercellularity, dysplasia of cellular elements, and consequent inadequate hematopoiesis, with resultant peripheral blood cytopenias.
Leukemia
Latest News
Advertisement
Advertisement
The review by Dr. Akhtari outlines the diagnosis, prognosis, and treatment options for patients with myelodysplastic syndromes (MDS), and touches on the current challenges in treating patients suffering from MDS.
This review will cover the key elements of modern acute lymphoblastic leukemia treatment regimens, focusing primarily on front-line treatment and concluding with a brief discussion of the management of relapsed disease.
We have witnessed remarkable gains in the biological understanding and treatment of acute lymphoblastic leukemia (ALL) over the past decade.
About 35 years ago, I encountered several children and adolescents with acute lymphoblastic leukemia or widespread non-Hodgkin lymphoma who presented with or who developed, upon initiation of therapy, severe renal and metabolic derangements.
Dr. Sonali Smith discusses the newest developments in the treatment of CML.
Dr. Jorge Cortes discusses new data on bosutinib, a new tyrosine kinase inhibitor for CML.
The accurate and in-depth documentation of learning gaps is a fundamental aspect of developing continuing education activities. To obtain a better understanding of community-based medical oncology practice patterns, 43 oncologists within the United States were recruited to complete a traditional clinical case–based questionnaire and to contribute specific anonymous demographic and treatment information derived from their actual patients. This information was used to create a cross-sectional case database on two types of cancer in which major clinical advances have been reported in recent years - multiple myeloma and follicular lymphoma. These diseases also are similar in that most patients experience clinically meaningful benefits from systemic treatment but are unlikely to be cured by therapy. As further described in this and the subsequent two articles, this case-based series documents that (a) clinical research advances are being quickly implemented in daily patient care and that (b) although therapeutic strategies vary based on patient age, the short-term outcomes in terms of response to and tolerance of treatment are similar in younger and older patients.
At a median follow-up of 36 months, multiple survival rates were nearly perfect at 99%. The leader of the Italian study called the low number of treatment failures reassuring news as to the durability of nilotinib response at three years post-therapy

The median reductions in Bcr-Abl transcripts at one year were greater with dasatinib (Sprycel) than with imatinib (Gleevec), according to the results of an intergroup phase II trial. A better molecular response should eventually correlate with better outcomes, making dasatinib a serious contender for upfront therapy in CML.
The likelihood of patients achieving complete cytogenetic response at any time was 1.5 times higher with dasatinib (Sprycel) than with imatinib (Gleevec), according to an investigator with the DASISION trial.
Nplate sustains platelet counts in patients with adult chronic immune (idiopathic) thrombocytopenic purpura (ITP) while single-dose Zevalin offers survival advantage in non-Hodgkin’s lymphoma.
The 24-month follow-up data from the ENESTnd trial showed that patients treated with nilotinib (Tasigna) had significantly better response rates and significantly lower rates of progression to accelerated phase or blast crisis when on treatment

Patients with early-stage Hodgkin’s lymphoma and a favorable prognosis can be treated with less intensive chemotherapy and radiotherapy regimens without affecting outcomes. This is the first study to show that less intensive therapy can be used without sacrificing benefits, according to lead author Andreas Engert, MD, and colleagues.

Here we present the case of a 3-year-old girl with generalized lymphadenopathy and fever, in whom the cause of the symptoms was initially thought to be infectious. Ultimately, however, anaplastic large cell lymphoma (ALCL) was diagnosed. Using this case as a backdrop, we discuss the wide range of systemic illnesses that the differential diagnosis of generalized lymphadenopathy encompasses.
Bruce Cheson, MD, has become chair of the Lymphoma Research Foundation Scientific Advisory Board. Dr. Cheson is professor of medicine, head of hematology, and director of hematology research at the Lombardi Comprehensive Cancer Center at Georgetown University Hospital in Washington DC. His two-year term as chair began in July 2010.

Drug is indicated for the treatment of patients with cutaneous T-cell lymphoma (CTCL) who have received at least one prior systemic therapy.
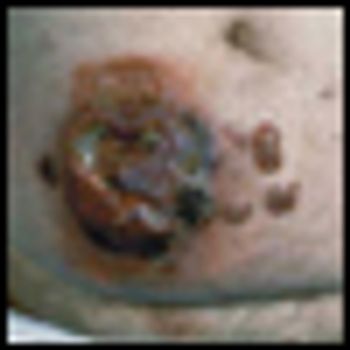
Anaplastic large cell lymphoma (ALCL) is a biologic and clinically heterogenous subtype of T-cell lymphoma. Clinically, ALCL may present as localized (primary) cutaneous disease or widespread systemic disease. These two forms of ALCL are distinct entities with different clinical and biologic features. Both types share similar histology, however, with cohesive sheets of large lymphoid cells expressing the Ki-1 (CD30) molecule. Primary cutaneous ALCL (C-ALCL) is part of the spectrum of CD30+ lymphoproliferative diseases of the skin including lymphomatoid papulosis. Using conservative measures, 5-year disease-free survival rates are>90%. The systemic ALCL type is an aggressive lymphoma that may secondarily involve the skin, in addition to other extranodal sites. Further, systemic ALCL may be divided based on the expression of anaplastic lymphoma kinase (ALK) protein, which is activated most frequently through the nonrandom t(2;5) chromosome translocation, causing the fusion of the nucleophosmin (NPM) gene located at 5q35 to 2p23 encoding the receptor tyrosine kinase ALK. Systemic ALK+ ALCLs have improved prognosis compared with ALK-negative ALCL, although both subtypes warrant treatment with polychemotherapy. Allogeneic and, to a lesser extent, autologous stem cell transplantation play a role in relapsed disease, while the benefit of upfront transplant is not clearly defined. Treatment options for relapsed patients include agents such as pralatrexate (Folotyn) and vinblastine. In addition, a multitude of novel therapeutics are being studied, including anti-CD30 antibodies, histone deacetylase inhibitors, immunomodulatory drugs, proteasome inhibitors, and inhibitors of ALK and its downstream signaling pathways. Continued clinical trial involvement by oncologists and patients is imperative to improve the outcomes for this malignancy.
Peripheral T-cell lymphomas (PTCLs) are rare and heterogeneous non-Hodgkin lymphomas that have been separated by clinical presentation, histology, immunohistochemistry markers, infectious agents, and genetic abnormalities. They may have extranodal dissemination and are often aggressive, especially when they express cytotoxic markers. The international T-cell Non-Hodgkin Lymphoma Study Group collaboration has highlighted differences in the frequency of these entities in different geographic areas.[1,2] For example, HTLV-1+ adult T-cell lymphomas are found in Japan and nasal NK/T-cell lymphoma occurs predominantly in Asian countries. The most common PTCLs are unique and not able to be classified by a specific marker or tumor antigen, and are known as peripheral T-cell lymphomas, not otherwise specified (PTCL-NOS).
Polymerase Chain Reaction (PCR) testing for BCR-ABL has become the primary method used to monitor leukemia levels in CML patients. As a CML patient for almost 5 years, and someone who is in regular contact with other CML patients from around the world, I continually see the confusion that surrounds this very important issue.
A multi-institutional group of researchers have zeroed in on a more accurate way to decipher treatment outcomes in young leukemia patients using information from a simple complete blood count test.
Parents and their children need to understand that advancing science does not always go hand-in-hand with a direct benefit to the patients.
Mycosis fungoides (MF), the most common cutaneous T-cell lymphoma, is a low-grade cutaneous lymphoma characterized by skin-homing CD4+ T cells. It is notable for highly symptomatic progressive skin lesions, including patches, plaques, tumors, and erytheroderma, and has a poorer prognosis at later stages. Diagnosis remains difficult owing to MF’s nonspecific skin presentation and identification of the optimal treatment strategy is challenging given the paucity of controlled trials and numerous and emerging treatment options. Management includes topical therapy with the addition of systemic therapy for patients with later-stage disease including tumors; erythroderma; and nodal, visceral, or blood involvement. Topical therapies include mechlorethamine (nitrogen mustard), carmustine (BCNU), steroids, bexarotene gel (Targretin Gel), psoralen plus ultraviolet A (PUVA), ultraviolet B (UVB), and either localized or total skin electron radiotherapy. Systemic therapies include interferon, retinoids, oral bexarotene (Targretin), denileukin diftitox (Ontak), vorinostat (Zolinza), extracorporeal photochemotherapy (photopheresis), and cytotoxic chemotherapy. Herein, we outline clinically relevant aspects of MF, including clinical presentation, pathology, diagnosis, and staging. We describe in detail existing and emerging therapeutics and offer specific recommendations for management of each stage of MF.
The article entitled “Diagnosis and Management of Mycosis Fungoides” by Shira Galper, Benjamin Smith, and Lynn Wilson is an excellent contemporary summary of the workup and management of mycosis fungoides (MF) and its leukemia variant, Sézary syndrome (SS). In their discussion of the diagnosis and staging of MF and SS, the authors include a discussion of proposed revisions by the International Society for Cutaneous Lymphoma and the European Organisation for the Research and Treatment of Cancer (ISCL/EORTC) which seek to identify prognostic subgroups. In addition, there is a complete overview of the various treatment options for management of MF and SS. This treatment overview closely parallels the 2010 National Comprehensive Cancer Network (NCCN) Practice Guidelines for MF and SS.
Galper et al. should be commended for their concise and useful review of the diagnosis and management of mycosis fungoides (MF). It is notable that all of the authors are radiation oncologists. While the reader may expect a radiation oncologist’s perspective on the management of mycosis fungoides, their review goes beyond highlighting the various radiation techniques used in the treatment of MF. It highlights the major diagnostic dilemmas when evaluating patients with skin lesions that eventually are diagnosed as MF or its leukemic counterpart, Sézary syndrome (SS). It also stresses the importance of a multidisciplinary approach in diagnosing and caring for MF patients involving dermatology, dermatopathology, radiation oncology, and hematology/oncology, and provides a concise review of the treatment options in the MF and SS armamentarium. Navigating these options requires a good understanding of the natural history of the disease, the side effects of treatment, the expected response rates of treatment, the median time to response, the patient’s comorbid conditions, and goals of care.
Advertisement
Advertisement
Trending on CancerNetwork
1
AI and MRD Take Center Stage on Day 2 of ASCO Breakthrough 2026
2
Sigvotatug Vedotin Does Not Significantly Improve Survival in NSCLC Trial
3
Cellular Therapy and Antibody-Drug Conjugates Shape Day 1 of ASCO Breakthrough 2026
4
41 Unexpected While Expecting: Rare Case of Pregnancy Associated Xanthogranulomatous Mastitis Masquerading as Malignancy
5