















































































More than 90% of women about to undergo a mammography were unable to accurately quantify their risk for breast cancer, either over- or underestimating their risk, according to the results of a large-scale survey presented at the ASCO Breast Cancer Symposium 2013.
Breast Cancer
Latest News
Advertisement
Advertisement
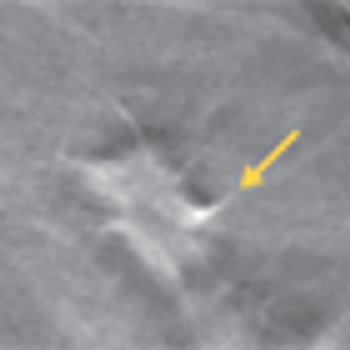
Expert radiologists were able to screen magnetic resonance images and rule out breast cancer diagnosis with a negative predictive value of about 99% using an abridged breast MRI protocol in a single-center study presented Saturday at the ASCO Breast Cancer Symposium 2013.

As part of our coverage for the ASCO Breast Cancer Symposium 2013, we spoke with Dr. Susan K. Boolbol, chief of the division of breast surgery at the Appel-Venet Comprehensive Breast Service at Beth Israel Medical Center in New York City, who is chairing a general session panel discussion on the overdiagnosis of breast cancer.
Results of the PrefHer study indicated that when given the option between subcutaneous trastuzumab and intravenous trastuzumab, significantly more patients with HER2-positive breast cancer preferred the subcutaneous administration.
A retrospective analysis of the HERA trial indicated that young age was not associated with early recurrence in women with HER2-positive breast cancer, despite previous research suggesting that young age at diagnosis might be a risk factor for recurrence and death.
To make the punishment fit the crime, you would want the decision of whether or not to use adjuvants to be informed by the degree of risk that the DCIS would recur. What factors can predict for an increased risk of recurrence, or more importantly, the risk of an invasive breast cancer occurring?

Use of calcium-channel blockers for treatment of high blood pressure for more than 10 years can increase the risk of breast cancer for women after menopause, a new study shows.
A study defining patterns of recurrence in node-negative breast cancer patients could help guide surveillance recommendations and future therapeutic approaches.
A new study shows that the combination of digital mammography plus tomosynthesis results in fewer false positive results compared with digital mammography alone. Women under the age of 50 and those with dense breasts had the greatest benefit from the combined screening approach.
Using easy-to-obtain risk factors for breast, ovarian, and endometrial cancers, researchers have come up with models that can predict an individual woman’s absolute risk for developing each type of cancer.
The combination of the chemotherapy capecitabine with external beam radiation was found to be both safe and effective in treating pain from bone metastases in patients with advanced breast cancer.
The American Society of Clinical Oncology (ASCO) has updated its guidelines on treating women at high risk of developing breast cancer with pharmacologic drugs.

Last week, the FDA announced that it would grant priority review to pertuzumab (Perjeta), as a neoadjuvant treatment for women with HER2-positive early-stage breast cancer.
The expression levels of two genes could indicate whether a woman with estrogen receptor-positive breast cancer is at risk for recurrence after 5 years of tamoxifen therapy and should receive subsequent therapy.

A 6-month regimen of treatment with trastuzumab for HER2-positive breast cancer failed to show noninferiority with the standard 12-month treatment regimen after 3.5 years of follow-up in the open-label, randomized, phase III PHARE trial.

The addition of everolimus (Novartis) to combination trastuzumab/vinorelbine leads to a significant improvement in progression-free survival compared with placebo in advanced and metastatic HER2-positive breast cancer.
Researchers from the Mayo Clinic have identified variants in two genes that result in a higher chance that tamoxifen or raloxifene will actually prevent breast cancer. More studies are needed, but if confirmed, women with these variants may be more likely to undergo the 5-year preventive regimen.
A high baseline level of soluble human epidermal growth factor receptor 2 (sHER2) was a prognostic indicator of shorter disease-free survival among patients with early-stage HER2-positive breast cancer, according to results from the North Central Cancer Treatment Group adjuvant trial N9831.

The use of a yoga program helped to reduce symptoms of insomnia among women with breast cancer undergoing hormonal therapy, and also resulted in an improved quality of life, according to new data presented at ASCO.

The goals of care for patients with hormone receptor (HR)-positive advanced breast cancer include prolongation of disease-free and overall survival, amelioration of symptoms, and improvement in quality of life.
Collaboration between oncologists and reproductive endocrinologists/infertility specialists not only will improve patient care, but it also will facilitate advances in the field through cooperative research and education.
Counseling a woman with breast cancer regarding fertility ideally attempts to align two goals-one for the patient and her disease, and one for the chance of a future child. Early collaboration with a reproductive specialist should enhance discussion of the most practically available fertility-promoting options.

A considerable number of women with breast cancer are diagnosed during their reproductive years. In the short period of time in which newly diagnosed women will need to make decisions about surgical options and adjuvant therapy, younger women with breast cancer also face the potential impairment or complete loss of their fertility.
The Case: A 48-year-old perimenopausal woman noted a lump in her left breast. She had had a mammogram 9 months earlier without abnormality. After ultrasound imaging confirmed a solitary mass measuring about 1.5 cm, a core needle biopsy demonstrated a poorly differentiated mammary carcinoma with chondroid features.

The Supreme Court announced a unanimous 9-0 decision that genes cannot be patented. After a long legal battle, the high court ruled against Myriad’s patents on two breast cancer susceptibility genes-BRCA1 and BRCA2-declaring that genes are products of nature and cannot be treated as inventions.
Advertisement
Advertisement
Trending on CancerNetwork
1
Where Does LAG-3/PD-1 Inhibition Fit In PD-1–Refractory Hodgkin Lymphoma?
2
VS-7375 Exhibits Activity in KRAS G12D–Mutated Solid Tumors
3
Offering Hope and Support Toward the Cancer Survivorship Journey
4
GLP-1 Receptor Agonists Reduce Colorectal Cancer Risk in IBD Populations
5