

















































































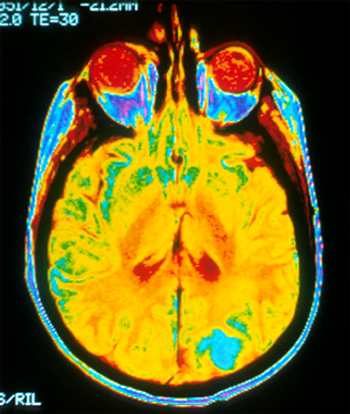
The diagnosis of central nervous system (CNS) recurrence is a much dreaded outcome among breast cancer patients, and its incidence varies with disease stage and cancer subtype.
The diagnosis of central nervous system (CNS) recurrence is a much dreaded outcome among breast cancer patients, and its incidence varies with disease stage and cancer subtype.

CancerNetwork speaks with Patricia S. Steeg, PhD, who has recently written a perspective in the journal Nature calling for a shift in both the types of drugs that are developed for breast cancer and in the way clinical trials are designed and executed.
The last two decades have seen the development of a variety of novel therapeutic agents that have improved prognoses for women with breast cancer.
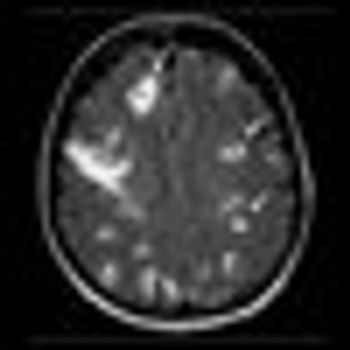
In this issue of ONCOLOGY, Drs. Lim and Lin present a comprehensive and up-to-date review of the basic biology of breast cancer brain metastasis (BCBM) and of emerging strategies for treating this increasingly common complication of advanced breast cancer (BC) (BC is second only to non–small-cell lung cancer in the frequency of central nervous system [CNS] metastasis.)

CancerNetwork speaks with Dr. Sara Hurvitz, director of the breast cancer program at the University of California in Los Angeles. Dr. Hurvitz is actively involved in translational phase I/II breast cancer clinical trials as well as in research to better define distinct types of breast tumors to better design novel targeted therapies.
One of the largest whole-exome sequencing analyses in breast cancer is published this week in Nature, identifying a new gene fusion among a subset of triple-negative breast cancers.

CancerNetwork and the journal ONCOLOGY present an exclusive interview with Dr. Kimberly Blackwell, Duke Cancer Institute, who discusses some of the most important information to come out of this year’s meeting and talks about the future of breast cancer research.
In this article, we review the current guidelines for adjuvant endocrine therapy in both premenopausal and postmenopausal women, and we discuss the clinical trials that were used to develop these guidelines.
The direction of research into adjuvant systemic therapy for breast cancer has been determined in large part by historical and cultural differences between Europe and the United States
The review by Drs. Ruta Rao and Melody Cobleigh in this issue of ONCOLOGY summarizes the state-of-the-art adjuvant hormonal therapy for breast cancer concisely and appropriately.

Pertuzumab has been approved in combination with trastuzumab (Herceptin) and docetaxel chemotherapy for women whose breast cancer overexpress the HER2 receptor and who have not received prior systemic treatment.

Researchers have found that circulating tumor cells can predict early recurrence and decreased overall survival in nonmetastatic breast cancer patients who have not yet been treated with chemotherapy.
The results of a randomized phase III trial show paclitaxel beat two newer chemotherapies, nab-paclitaxel and ixabepilone in the treatment of metastatic breast cancer patients who have not had prior systemic therapies.
Women previously treated for HER2-positive breast cancer have lower rates of relapse when given a novel peptide vaccine. The AE37 vaccine showed a 43% risk reduction in these patients after 22 months of follow-up in a phase IIb clinical trial.

Women with metastatic HER2-positive breast cancer treated with a taxane-based chemotherapy in combination with trastuzumab as a first-line of treatment have a longer progression-free survival compared to chemotherapy in combination with lapatinib (Tykerb)
A 13-gene signature can predict the development of brain metastasis among patients with advanced HER2-positive breast cancer who have estrogen-receptor (ER)-negative tumors. The results were presented at a breast cancer session at the 2012 meeting of the American Society of Clinical Oncology.
Results of a large phase III trial shows that a new oncology therapy, trastuzumab emtansine (T-DM1), significantly delays progression of disease in women with HER2-positive advanced breast cancer previously treated with a taxane chemotherapy and trastuzumab (Herceptin).

The first randomized, controlled clinical trial testing the effect of weight loss on sex hormone levels in overweight, postmenopausal women shows a benefit with moderate weight loss.
As Smith et al[1] discuss, randomized controlled trials (RCTs) have shown that mammography reduces deaths due to breast cancer across ages 40 through 74 years, and within subsets by decade.[2]
Drs. Smith, Duffy, and Tabár provide an excellent history of breast cancer screening, including a summary of the randomized trials, the technical approaches, and the range of recommendations for screening.
In this paper, the historic and recent evidence supporting the value of breast cancer screening will be described, along with the underpinnings of the current debate over the relative and absolute benefit of regular mammography screening.

A new study from the National Cancer Institute shows that physical activity is associated with lower mortality rates in patients with breast and colon cancers.

An abstract presented at the 13th Annual Meeting of the American Society of Breast Surgeons suggests that women who are at high risk for recurrence may not need a mastectomy.

New data presented at the 13th Annual Meeting of the American Society of Breast Surgeons shows radiofrequency ablation can prevent local breast cancer recurrence just as effectively as radiation therapy. Compared to radiation therapy, radiofrequency ablation showed superior cosmetic results and poses little risk to healthy tissue.

A study published today shows that whole-breast irradiation fares better than brachytherapy for women with breast cancer.