

















































































Combination treatment with the PARP inhibitor olaparib plus the PI3K inhibitor BKM120 showed a benefit in subsets of breast cancer and ovarian cancer patients.
Combination treatment with the PARP inhibitor olaparib plus the PI3K inhibitor BKM120 showed a benefit in subsets of breast cancer and ovarian cancer patients.
In an ongoing study, the immunotherapy MPDL3280A continues to be well-tolerated and to show signs of activity in triple-negative breast cancer patients.

Women who spend less time eating each day and an increased amount of hours fasting overnight had a decreased risk of breast cancer.

No benefit of axillary lymph node evaluation has been shown for women with DCIS, yet this lymph node analysis is still often performed in these patients.
A recent retrospective study elucidates the correlation between breast cancer subtype and metastasis site, time to relapse, and patient survival.

Women with diabetes are at a greater risk of being diagnosed with advanced-stage breast cancer, according to a retrospective study.
A major change in the clinical management of breast cancer, most early-stage patients now have sentinel node dissection as opposed to full lymph node removal.

Women who received cognitive behavioral stress management after surgery for early breast cancer reported better quality of life and lower symptoms of depression.

In this interview we discuss the current guidelines for lymph node staging in breast cancer and dive into the debate surrounding sentinel node biopsies.
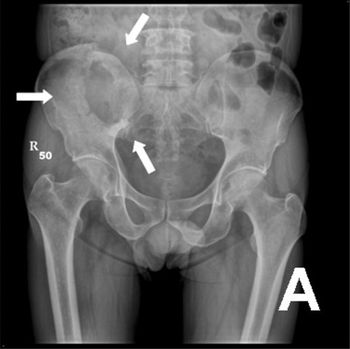
Researchers were able to demonstrate response to radiotherapy in breast cancer patients with osteolytic metastases by measuring increases in bone density.
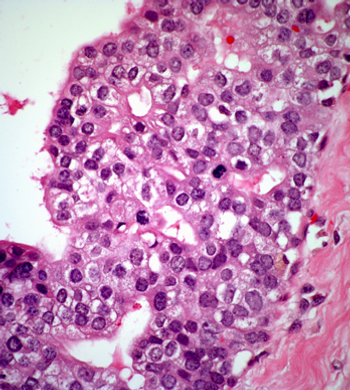
While pathologists usually agree on healthy and malignant breast tissue from biopsy slides, there is less agreement on samples that fall somewhere in the middle.
Women with a first-degree relative diagnosed with prostate cancer may be at increased risk for developing breast cancer, according to a new study.

The idea that breast cancer is overdiagnosed is being perpetuated in an effort to reduce access to breast cancer screening, according to a presentation at MBCC.
As more treatment options become available for metastatic HER2-positive breast cancer, some questions regarding the optimal sequencing of therapies remain.

The risk of early, sudden-onset menopause in women treated for early-stage breast cancer can be reduced with goserelin, a gonadotropin-releasing hormone agonist.
A physician’s age may have an effect on his or her opinions about the effectiveness of breast cancer screening methods, including self-exam and mammography.

Women with hormone receptor-positive breast cancer may be more scared, anxious, or concerned about treatment-related adverse events and cancer symptoms.
Women with breast cancer who received first-line eribulin were able to stay on treatment longer and had better outcomes when they received dose modifications.
According to a presentation at MBCC, modern breast cancer staging systems should include grade, estrogen receptor status, and possibly other biologic markers.

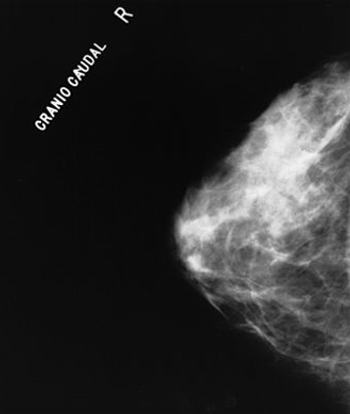
At MBCC, one presenter made the argument for screening mammography for all women starting at the age of 40, despite the controversy surrounding the topic.

As part of our MBCC coverage, we discuss how physicians can improve the patient experience through pain control both during and after breast cancer treatment.

As part of our MBCC coverage we discuss MRI screening for breast cancer in patients who carry a BRCA mutation or have a first-degree relative who is a BRCA carrier.
Economic factors, including household income, and racial disparities both play a role in the adherence to hormonal therapy in breast cancer patients.

The addition of bevacizumab to endocrine therapy did not prolong survival in postmenopausal women with advanced HER2-negative, HR–positive breast cancer.
An inhibitor of osteoclast formation can stop the proliferation of dormant tumor cells that in some breast cancer survivors turn into bone metastases.