Articles by William J. Gradishar, MD

TIP136 ELEGANT: Elacestrant Versus Standard Endocrine Therapy (ET) in Women and Men With Node-Positive, Estrogen Receptor–Positive (ER+), HER2-Negative (HER2–), Early Breast Cancer (eBC) With High Risk of Recurrence in a Global, Multicenter, Randomized, Open-Label Phase 3 Study
ByAditya Bardia, MD, MPH, FASCO,Virginia Kaklamani, MD, DSc,Joyce O’Shaughnessy, MD,Peter Schmid, MD,J. Thaddeus Beck,Michelino De Laurentiis,Giuseppe Curigliano,Hope S. Rugo, MD,Carlos H. Barcenas,William J. Gradishar, MD,Michail Ignatiadis,David Cameron,Giulia Tonini,Simona Scartoni,Jennifer Crozier,Tomer Wasserman,Sara M. Tolaney, MD, MPH 
Panel Reflections and Future Directions in Breast Cancer Care
ByHeather McArthur, MD, MPH,Sarah Sammons, MD,Ruta Rao, MD,William J. Gradishar, MD,Tiffany Traina, MD, FASCO Panelists discuss how the expanding volume of clinical data—both positive and negative—is increasing treatment complexity while reinforcing the need for individualized, patient-centered decision-making.
Toxicity Management, Monitoring, and Quality-of-Life Concerns
ByHeather McArthur, MD, MPH,Sarah Sammons, MD,Ruta Rao, MD,William J. Gradishar, MD,Tiffany Traina, MD, FASCO Panelists discuss how toxicity monitoring and quality-of-life considerations must be adapted as potent therapies move into earlier-line and curative-intent settings.
High-Risk Populations, Patient Selection, and Advancements in Maintenance Therapy – Insights from Her2Climb05
ByHeather McArthur, MD, MPH,Sarah Sammons, MD,Ruta Rao, MD,William J. Gradishar, MD,Tiffany Traina, MD, FASCO Panelists discuss how identifying high-risk subgroups enables more precise selection of maintenance therapies that maximize progression-free survival while accounting for biomarker differences.
Optimizing HER2-Positive Disease Management: Neoadjuvant, Adjuvant, and Maintenance Advances
ByHeather McArthur, MD, MPH,Sarah Sammons, MD,Ruta Rao, MD,William J. Gradishar, MD,Tiffany Traina, MD, FASCO Panelists discuss how emerging neoadjuvant and adjuvant data in HER2-positive breast cancer are challenging traditional standards and supporting earlier use of highly effective agents.
Antibody Drug Conjugates in Hormone Receptor Positive Disease – ASCENT-07 and Beyond
ByHeather McArthur, MD, MPH,Sarah Sammons, MD,Ruta Rao, MD,William J. Gradishar, MD,Tiffany Traina, MD, FASCO Panelists discuss how results from antibody-drug conjugate trials, including those that fail primary endpoints, provide critical insights for refining sequencing strategies in hormone receptor–positive disease.
Post-CDK4/6 Endocrine Strategies and the evERA Trial
ByHeather McArthur, MD, MPH,Sarah Sammons, MD,Ruta Rao, MD,William J. Gradishar, MD,Tiffany Traina, MD, FASCO Panelists discuss how post-CDK4/6 endocrine strategies increasingly rely on molecular profiling to guide therapy selection and optimize benefit in resistant disease.
EMBER-3 and Progress in ESR1-Mutant Disease
ByHeather McArthur, MD, MPH,Sarah Sammons, MD,Ruta Rao, MD,William J. Gradishar, MD,Tiffany Traina, MD, FASCO Panelists discuss how data from recent ESR1-mutant disease trials are influencing interpretation of survival end points, regulatory expectations, and real-world adoption of oral SERDs.
Guideline Perspectives and the Shift Toward Earlier ADC Integration
ByHeather McArthur, MD, MPH,Sarah Sammons, MD,Ruta Rao, MD,William J. Gradishar, MD,Tiffany Traina, MD, FASCO Panelists discuss how rapidly evolving guidelines are reshaping treatment pathways by preserving endocrine therapy as a backbone while introducing earlier use of combination regimens and ADCs.
Sequencing Targeted Therapies and Approaches for Genomic Versus Non-Genomic Cases
ByHeather McArthur, MD, MPH,Sarah Sammons, MD,Ruta Rao, MD,William J. Gradishar, MD,Tiffany Traina, MD, FASCO Panelists discuss how sequencing targeted therapies after CDK4/6 inhibitors differs for patients with actionable mutations versus those without, incorporating evidence for rechallenge and combination strategies.
Introduction and Genomic Testing in Advanced Breast Cancer
ByHeather McArthur, MD, MPH,Sarah Sammons, MD,Ruta Rao, MD,William J. Gradishar, MD,Tiffany Traina, MD, FASCO Panelists discuss how integrating both tissue and liquid genomic testing at diagnosis and progression improves detection of tumor heterogeneity and informs personalized treatment decisions in metastatic breast cancer.

TPS 28 ELEGANT: Elacestrant VS Standard Endocrine Therapy in Women and Men With Node-Positive, Estrogen Receptor-Positive, HER2-Negative, Early Breast Cancer With High Risk of Recurrence in a Global, Multicenter, Randomized, Open-Label Phase 3 Study
ByAditya Bardia, MD, MPH, FASCO,Virginia Kaklamani, MD, DSc,Joyce A. O’Shaughnessy,Peter Schmid, MD,J. Thaddeus Beck,Michelino De Laurentiis,Guiseppe Curigliano,Hope S. Rugo, MD,Carlos Barcenas,William J. Gradishar, MD,Michail Ignatiadis,David Cameron,Giulia Tonini,Simona Scartoni,Jennifer Crozier,Leo Viana Nicacio,Tomer Wasserman,Sara M. Tolaney, MD, MPH TPS 38 ELCIN: Elacestrant in Women and Men With CDK4/6 Inhibitor-Naive Estrogen Receptor-Positive, HER2-Negative Metastatic Breast Cancer: An Open-Label, Multicenter, Phase 2 Study
ByVirginia Kaklamani, MD, DSc,Giorgi Dzagnidze,Nicoleta Zenovia Antone,Anu Thummala,Mikheil Janjalia,Patricia Santi,Carlos Barrios,Mehmet Ali Nahit Sendur,Xiaoling Zhang,Angela Gambioli,Manuel Dominguez,Kathy Puyana Theall,Tomer Wasserman,William J. Gradishar, MD 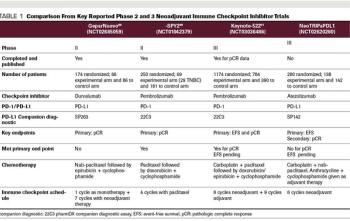
Experts review the current landscape and potential use of neoadjuvant chemotherapy with additional novel agents for patients with localized TNBC.

This video highlights an education session from SABCS on the management of locoregional recurrence in breast cancer.
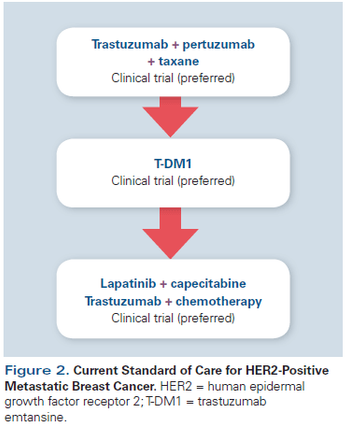
This review will summarize the current standard of care; key issues that arise when treating patients with HER2-positive disease; and developments in novel therapeutics, including small-molecule inhibitors, nanoparticles, immunotherapy, and agents targeting resistance pathways.

In this interview we discuss the effect of breast cancer treatments on fertility and the role oncologists can play in facilitating fertility care for their patients.

Here, we provide an in-depth review of the current evidence for the addition of ovarian suppression to adjuvant endocrine therapy, and we offer recommendations for clinical management.
In addition to the direct effects of primary tumors in bone, bone complications in cancer patients occur from metastasis to bone and through the effects of cancer-related treatments and conditions. Bone is a very common metastatic site for many cancers, including myeloma, melanoma, and breast, prostate, thyroid, lung, bladder, and kidney cancers. Metastatic bone lesions can be osteolytic (bone destruction resulting from increased bone resorption and reduced formation), osteoblastic (increased bone formation), or both.
Progress continues in the investigation of cytotoxicchemotherapy for breast cancer, and recentdata have yielded important new insights.
The use of adjuvant endocrinetherapy in early-stage breastcancer is thought to eradicatemicrometastatic disease that may leadto systemic recurrences. Until relativelyrecently, the standard adjuvantendocrine therapy option was tamoxifen.Data from the Early Breast CancerTrialists’ Collaborative Group(EBCTCG) overview analysis reporteda 50% reduction in the risk of relapseand a 28% reduction in the riskof death in estrogen receptor (ER)-positive patients treated with 5 yearsof tamoxifen.[1] This benefit was observedregardless of menopausal orlymph node status and whether or notpatients were receiving chemotherapy.There was no such benefit documentedin ER-negative cancersreceiving tamoxifen. Tamoxifen hasalso been associated with a 47% reductionin the risk of developing contralateralbreast cancer.[1]
With the advent of aromataseinhibitor use in the adjuvantsetting,[1] and the inceptionof trials examining their usefor breast cancer prevention, it seemsprudent to evaluate what we know todate about the long-term effects of these agents. Unfortunately, unlike selectiveestrogen-receptor modulators(SERMs)-in particular tamoxifen,[2]which has been used for over 15 yearsin patients with early-stage breast cancer-long-term data on the use of aromataseinhibitors are minimal.
Tamoxifen (Nolvadex), a selective estrogen-receptor modulator, or SERM, is currently the endocrine therapy of choice for all stages of hormone-responsive breast cancer. Only tamoxifen has been approved by the US Food and
Book Review: Textbook of Uncommon Cancer, Second Edition
ByDerek Raghavan, MD, PhD, FACP, FRACP, FASCO,Martin L. Brecher, MD,David H. Johnson, MD,Neal J. Meropol, MD,Paul L. Moots, MD,J. Tate Thigpen, MD,William J. Gradishar, MD The second edition of the Textbook of Uncommon Cancer is a useful resource for practicing oncologists who encounter unusual presentations of common tumors or esoteric subtypes of more common cancers. The text is laid out according to
New treatment strategies for advanced breast cancer have focused on both the development of new molecular targets in breast cancer cells, as well as improving the therapeutic index of presently available therapy. The
Symptoms related to estrogen deficiency are among the most common complaints that postmenopausal breast cancer patients bring to the attention of oncologists. Menopause develops in these patients either naturally or prematurely as a result of cancer chemotherapy and/or endocrine therapy.
Optimal management of locally advanced breast cancer (stage III) generally includes a combination of primary chemotherapy followed by surgery (if feasible), and local radiotherapy and adjuvant chemotherapy with or
