




















































A new study evaluated whether busulfan and melphalan improve EFS and OS when given after vincristine, ifosfamide, doxorubicin, and etoposide induction.
A new study evaluated whether busulfan and melphalan improve EFS and OS when given after vincristine, ifosfamide, doxorubicin, and etoposide induction.
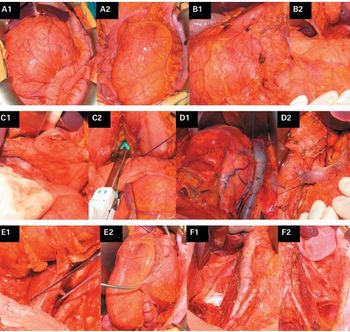
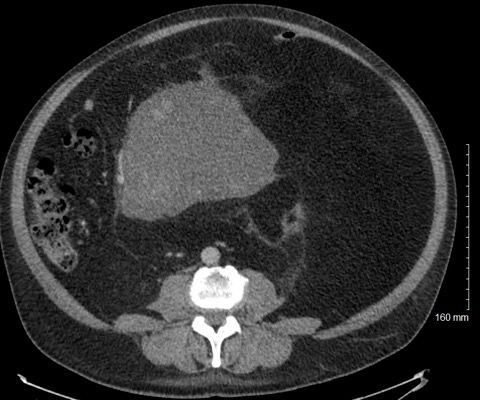
Retroperitoneal sarcoma is a rare tumor whose diagnosis and management can be challenging and for which management requires a multidisciplinary team.
Six months of maintenance chemotherapy improved OS in children with high-risk rhabdomyosarcoma.
Investigators have discovered that clofarabine and cladribine may be used as a targeted therapy in diseases where CD99 plays a critical role, including Ewing sarcoma and auto-immune disorders.
A comparison of margin classification systems revealed some differences in their ability to determine local recurrence risk for soft-tissue sarcoma.
The GPNMB-targeted agent known as glembatumumab vedotin was reasonably well tolerated and showed some activity in a phase II study of recurrent/refractory osteosarcoma, but this activity was not enough to continue the drug’s evaluation in this setting based on the study protocol.
An analysis of more than 800 patients found that the one-size-fits-all approach to “aftercare” for localized soft-tissue sarcoma is misguided. Local recurrence and distant metastasis occur in a non-constant fashion in the years after treatment, and a time- and risk-adapted strategy for aftercare is warranted.
Treatment with hyperthermia improved survival when added to neoadjuvant chemotherapy for patients with localized high-risk soft-tissue sarcoma.
Lurbinectedin demonstrated clear antitumor activity as a single agent in patients with advanced or relapsed Ewing sarcoma, according to results of a phase II trial.
The first phase II study of cabozantinib in soft-tissue sarcoma yielded several responses, including several subtypes such as alveolar soft-part sarcoma and myxoid liposarcoma.
The combination of durvalumab and tremelimumab offered a modest response rate in unselected patients with heavily pretreated metastatic sarcoma, but higher rates were seen in specific subtypes, including angiosarcoma and alveolar soft-part sarcoma.
NY-ESO-1 SPEAR T-cell therapy showed promising results and was reasonably safe in patients with synovial sarcoma, according to a new study. The addition of fludarabine may be important to achieving those positive results.
A phase II study found that the immunotherapy agent pembrolizumab has meaningful clinical activity in patients with two subtypes of advanced sarcoma.

In this interview we discuss the phase III trial of aldoxorubicin in patients with advanced soft-tissue sarcoma, which showed improved efficacy and reduced toxicity over doxorubicin.

We spoke with Mrinal M. Gounder, MD, about next-generation sequencing for sarcoma, and how it can be used to inform treatment decisions and prognosis.
Treatment with the PD-1 inhibitor pembrolizumab plus metronomic cyclophosphamide had limited activity in patients with soft-tissue sarcomas and gastrointestinal stromal tumors.
An experimental compound known as G100 may be a potentially viable agent for local control of metastatic soft tissue sarcomas.
In this review we discuss preoperative diagnosis and the role of pathology, and we summarize the current literature regarding the management of uterine sarcomas.
Survivors of childhood Ewing sarcoma have substantial risk for late mortality and subsequent neoplasms, according to a long-term follow-up study.
A genomic analysis of Ewing sarcoma found substantial epigenetic heterogeneity both between tumors and within tumors, highlighting the need to consider non-genetic aspects in cancer biology and treatment.
A study examining predictors of outcome following relapse of primary retroperitoneal sarcoma found that time to local recurrence or distant metastasis significantly predict survival, and that patients who undergo resection for the recurrent disease have better survival than others.
Angiosarcoma has generally poor survival among Asian patients; though chemotherapy can be effective, it has been underused in the last few decades.
Aldoxorubicin yielded significantly better progression-free survival over investigator’s choice of various chemotherapy options in patients with relapsed or refractory leiomyosarcoma and liposarcoma, according to updated results of a phase III trial.
In this slide show we highlight some of the top news on sarcoma in 2016, including the first frontline FDA approval in 40 years, and studies on imaging in Ewing sarcoma, maintenance chemotherapy in osteosarcoma, and more.
A case study found that a patient with an inflammatory myofibroblastic tumor and a chromoplectic TPM3-ALK rearrangement that may be involved in tumorigenesis had a strong response to the ALK inhibitor ceritinib.