

















































Survivors of sarcoma have significant long-term mortality from both second cancers and noncancer-specific causes when compared with the general population, a large study showed.
Sarcoma
Latest News

Advertisement
Advertisement
A recent review clarifies the major classification changes in the current 2013 WHO classification, and factors in new genetic data that has emerged since the publication of the current volume.
Combination treatment with ifosfamide and doxorubicin for advanced soft-tissue sarcoma did not improve overall survival compared with treatment with doxorubicin alone, despite improvements in both overall response and progression-free survival.

Pathologic and molecular features of gastrointestinal stromal tumors (GIST) were generally not correlated with outcome in a study involving adjuvant imatinib therapy following resection of the primary tumor.
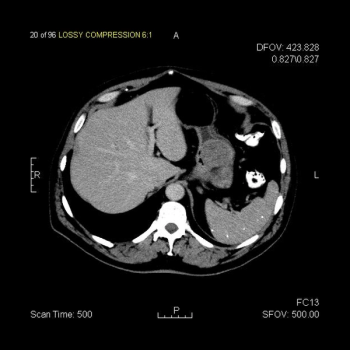
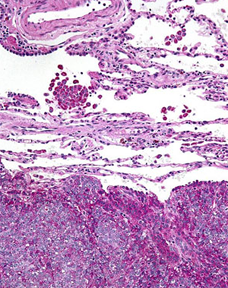
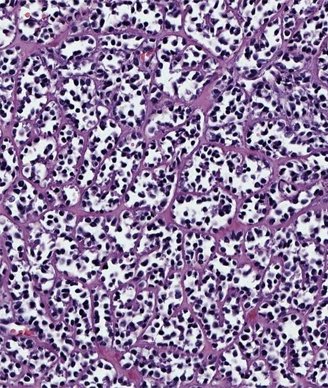
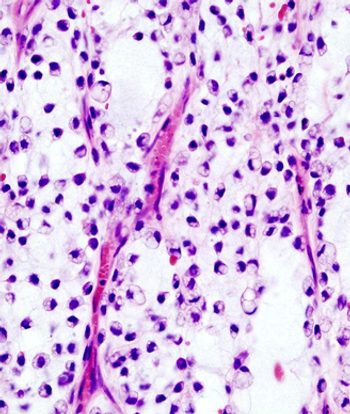
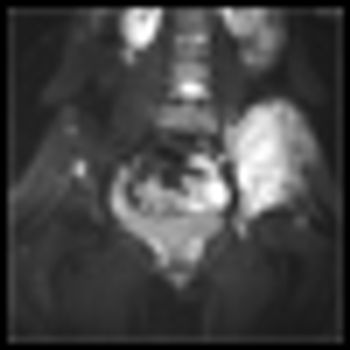
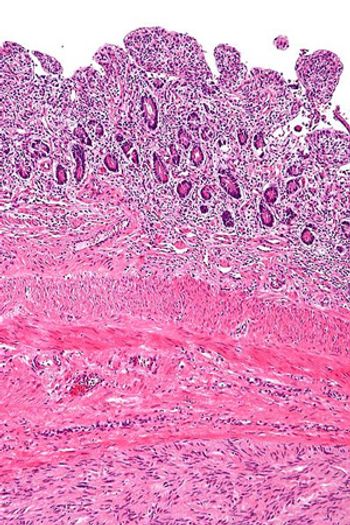
This slide show features a CT image, and pathology images of gastrointestinal stromal tumors (GISTs) arising in the stomach using H&E, CD34, and c-Kit staining.
The use of preoperative radiotherapy may be a reasonable approach to patients with borderline resectable soft-tissue sarcomas, according to the results of a retrospective study.
Single patients with soft-tissue sarcoma of the extremities had worse overall survival and were less likely to undergo several important treatment options compared with their married counterparts, according to results of a recent study.
A recent exploratory study found that GIST cells showed unexpected sensitivity to certain kinds of chemotherapy drugs not typically associated with the diseases’ treatment.
The results of a retrospective study indicated that patients with metastatic GIST who are able to achieve complete macroscopic surgical resection of their disease may be able to achieve long-term survival.
Researchers have identified several characteristics of long-term responders to pazopanib in patients with advanced soft-tissue sarcomas, including having a normal hemoglobin level at baseline.
Patients with retroperitoneal sarcomas who are unable to obtain complete resection after initial resection are left with few treatment options for palliative therapy, according to the results of a recent study.
Patients with heavily pretreated metastatic gastrointestinal stromal tumors were able to tolerate combined treatment with the pan-deacetylase inhibitor panobinostat and imatinib, according to the results of a small phase I study.
A phase II trial showed that patients with advanced gastrointestinal stromal tumors had a marginal response to pazopanib when assigned to the treatment after two or more failed therapies.
Results of a small study indicate that patients with gastrointestinal stromal tumors had increased activity of Src, but unlike in other tumors, it may be associated with longer overall survival.
The Akt/mammalian target of rapamycin (mTOR) pathway is often activated in patients with synovial sarcoma, and activation of the pathway is associated with worse outcomes, according to a new study.

The combination of palifosfamide and doxorubicin was no better than doxorubicin and placebo in the phase III PICASSO 3 trial of patients with metastatic soft-tissue sarcoma.
Carbon ion radiotherapy is a safe and effective method for treating unresectable spinal sarcomas, according to a retrospective analysis from one center in Japan.
The multikinase angiogenesis inhibitor pazopanib was well tolerated and exhibited some responses in pediatric patients with soft-tissue sarcomas and other refractory solid tumors in a phase I trial.
Almost half of the resections performed for deep and malignant extremity soft-tissue sarcomas are done by non-oncology surgeons including orthopedic surgeons and general surgeons, according to a new study.

Surgery is the mainstay of treatment for localized soft-tissue sarcoma (STS). It consists primarily of resection of the tumor along with a cuff of surrounding healthy tissue. In limb and trunk wall sarcomas, this basically implies resection of the surrounding soft tissues, which are mainly muscles, subcutaneous fat, and skin.[1] In the retroperitoneum, this necessarily should imply resection of adjacent viscera, even when they are not overtly involved.[2] This is the only way to avoid/minimize the presence of tumor cells at the cut surface (ie, positive microscopic surgical margins). Positive microscopic surgical margins are associated with a higher risk of local failure, distant metastases, and death.[3-6] Moreover, for STS located at critical sites, such as retroperitoneal sarcoma (RPS), positive surgical margins may have a direct impact on survival, favoring the development of inoperable local recurrences.[7] Indeed, unlike with STS arising in the extremities and trunk wall, local control in RPS poses a significant challenge and remains the leading cause of death, particularly in patients with low- to intermediate-grade tumors-roughly 75% of all cases.[8-13] Extending the resection to adjacent uninvolved viscera for primary RPS is the only way to minimize the presence of microscopic surgical margins and hence maximize the chance of cure. In essence, this strategy should often include ipsilateral nephrectomy and colectomy; locoregional peritonectomy and myomectomy (partial/total) of the muscle of the lateral/posterior abdominal wall (usually the psoas) (see Figure); splenectomy and left pancreatectomy, for tumors located on the left upper side; occasionally pancreaticoduodenectomy or hepatectomy, for tumors located on the right side; and vascular and bone resection only if vessels/bone are overtly infiltrated.[2]

Recently controversy has emerged regarding the extent of resection that constitutes optimal surgical management of retroperitoneal soft-tissue sarcoma.
The addition of adjuvant chemotherapy using doxorubicin, ifosfamide, and cisplatin, to pelvic radiation therapy for the treatment of uterine sarcomas increased 3-year disease-free survival in a group of women with localized disease, but also resulted in two toxic deaths among the study group.
Decreasing the time between cycles of standard chemotherapy for Ewing’s sarcoma from 3 weeks to 2 weeks increased event-free survival without an associated increase in toxicity, according to the results of a Children’s Oncology Group report.

Despite its place in standard practice, the performance of pulmonary metastasectomy in patients with sarcoma and lung metastases may not improve the survival rate of these patients, according to information from a systematic review of studies investigating the procedure in this patient population.
Treatment of gastrointestinal stromal tumor (GIST) with regorafenib after prior treatment failure with both imatinib and sunitinib resulted in a PFS survival benefit for patients across all prespecified subgroups.
Advertisement
Advertisement
Trending on CancerNetwork
1
Steel Particulate Matter Prompts Cyclophosphamide for Injection Recall
2
FDA Approves Blood-Based Test for Colorectal Cancer Screening
3
Belzutifan Combo Exhibits Comparable HRQoL Vs Cabozantinib in RCC
4
RP1's Long Road: A Timeline of RP1's Regulatory Journey in Advanced Melanoma
5