















































































Findings from the GOG-3007 study suggest everolimus plus letrozole might be effective in advanced persistent or recurrent endometrial carcinoma.
Endometrial Cancer
Latest News

Advertisement
Advertisement
Use of oral contraceptives may be beneficial for chemoprevention for a range of women with different baseline cancer risks, according to the results of a new study.
Two studies on Lynch syndrome highlight cancer screening and surveillance opportunities.

Women with increased levels of cadmium, which mimics estrogen in the body, had a higher risk of endometrial cancer, according to a recently published observational study.

The diagnostic benefits of SLN evaluation include an ability to identify the extent of tumor dissemination and the utility of SLN mapping in guiding targeted adjuvant treatment in high-risk patients.

The question that should be posed to those who advocate for lymphadenectomy as a tool to guide the adjuvant therapy of endometrial cancer is: At what cost to the patient is lymphadenectomy performed?
Intentional weight loss can lower the risk of endometrial cancer in postmenopausal women, according to a new study. This was especially true of obese women who lost weight.
Microsatellite instability analysis and immunohistochemistry analysis are highly concordant with regard to testing for mismatch repair deficiency in endometrial cancer.
After a review of the published literature, the panel voted on three variants to establish best practices for the utilization of imaging, radiotherapy, and chemotherapy after primary surgery for early-stage endometrial cancer.
A small study has found an increased risk for serous or serous-like endometrial carcinoma among women with BRCA1 mutations after undergoing risk-reducing salpingo-oophorectomy without hysterectomy.
Researchers were able to molecularly classify endometrial cancers with distinct survival differences using a new classification tool called ProMisE that uses clinically applicable methods.

While continuing to warn against use of laparoscopic power morcellators for the removal of uterus or uterine fibroids in most women, the FDA is allowing the marketing of a containment system for use with certain power morcellators to isolate tissue not suspected to be cancerous.
The combination of sentinel lymph node mapping and use of uterine intraoperative restrictive frozen section in patients with low-grade endometrial cancer can reduce the rate of complete lymphadenectomy without reducing the detection of lymphatic metastasis.
Loss of function of the PTEN tumor suppressor gene leads to resistance to therapies targeting the Notch signaling pathway according to a mouse study presented at the 2016 Society of Gynecologic Oncology annual meeting, held in San Diego, March 19-22, 2016.

According to a recent study, the use of oral birth control pills has prevented 200,000 cases of endometrial cancer over the last 10 years.
The addition of bevacizumab to carboplatin/paclitaxel chemotherapy increases progression-free survival in advanced/recurrent endometrial cancer patients.
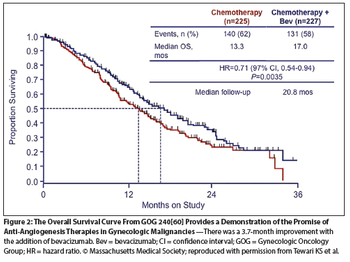
The purpose of this paper is to provide a review of site-specific treatment options that involve the targeting of angiogenesis in gynecologic malignancies.

Drinking coffee multiple times a day may decrease the risk of endometrial cancer in women, according to a new study.
Women with metabolic syndrome who are age 65 or older have an increased risk of endometrial cancer, according to the results of a new study.
An analysis of a large number of women suggested that those who use bisphosphonates, a bone medication used to treat osteoporosis and other bone loss diseases, have a reduced risk of endometrial cancer.

Researchers are estimating that about 3.6% of new cancer cases in 2012 in adults may be attributed to a high BMI, equating to about 481,000 new cancer cases.

The University of North Carolina has multiple posters accepted to the Gynecologic Oncology General Poster Session at this year’s ASCO meeting. Let’s take a virtual walk through several of these abstracts.
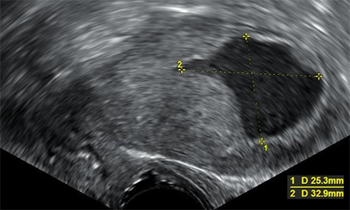
In this interview we discuss the diagnosis and treatment of endometrial cancer, a gynecologic cancer that forms in the tissue lining the uterus.

The Society of Gynecologic Oncology (SGO) recently issued two new clinical practice statements recommending genetic testing for all women with endometrial and ovarian cancers, regardless of family history.
As advances in treatment strategies continue to focus on individualization of therapy, the identification of disease subsets is crucial to strategizing optimal therapeutic approaches.
Advertisement
Advertisement
Trending on CancerNetwork
1
Where Does LAG-3/PD-1 Inhibition Fit In PD-1–Refractory Hodgkin Lymphoma?
2
Sigvotatug Vedotin Does Not Significantly Improve Survival in NSCLC Trial
3
VS-7375 Exhibits Activity in KRAS G12D–Mutated Solid Tumors
4
Offering Hope and Support Toward the Cancer Survivorship Journey
5