




















































































In my experience, being treated for low-volume Gleason 6 tumors is the norm, not the exception, for men in the United States. Surveillance may be discussed as an option, but it is not taken seriously.
Prostate Cancer
Latest News
Advertisement
Advertisement
The concept of active surveillance is based on the observation that Gleason 6 (pattern 3) prostate cancer is an indolent condition that poses little or no threat to the patient’s life. Conservative management is thus appropriate for these patients.
Further analyses of data subsets from the ALSYMPCA study of the alpha particle-emitting isotope Ra-223 (Xofigo) were presented at ASCO, providing additional evidence of efficacy and safety of the recently FDA approved therapeutic agent.
Addition of curcuminoids to treatment with docetaxel was well tolerated and showed promise in improving the response rate to docetaxel “in terms of both PSA decrease and objective response” in a phase II trial in patients with castration-resistant prostate cancer.
Monotherapy with enzalutamide (Xtandi) achieved a “high PSA response rate and marked PSA decline” in patients with hormone-naïve prostate cancer after 6 months in a single-arm, multicenter phase II study.
Treatment with 200 µmol per day of sulforaphane for 20 weeks was “feasible, safe,” and inhibited histone deacetylase (HDAC) function in a single-arm study of 20 patients who had non-castrate biochemical (PSA)-recurrence of prostate cancer despite surgery or radiation.

Ahead of the 2013 ASCO meeting we highlight some of this year's prostate cancer sessions, many of which focus on how best to use the new agents that have been approved recently, as well as looking into new drugs and combinations presented from early trials.

The AUA recently released its first set of treatment guidelines addressing the treatment of men with metastatic castration-resistant prostate cancer (mCRPC) at its 2013 Annual Meeting. The guidelines were released to address the increasingly complex treatment landscape available for patients with mCRPC.

Survival data of prostate cancer patients 70 and older show that those with three or more comorbidities and low- or intermediate-risk prostate cancer are less likely to die from prostate cancer than another health issue. But those with aggressive, high-risk disease are more likely to die from their prostate cancer.

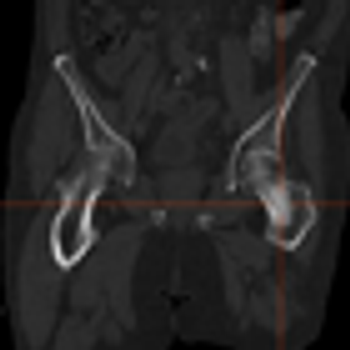
Palliative radiotherapy is an effective means of alleviating pain and improving overall quality of life in elderly patients with bone metastases, according to a new study.
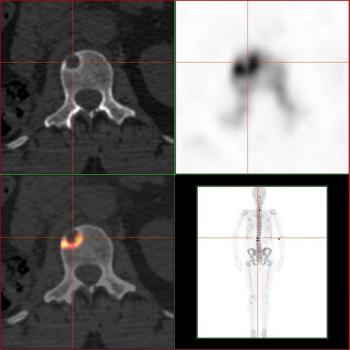
This slide show features images of diffuse osteoblastic bone metastases in a 70-year-old advanced prostate cancer patient, bone metastases in the vertebral column of a kidney cancer patient, and more.
The American Urological Association (AUA) released a new clinical guideline detailing recommendations for the use of prostate cancer screening in average-risk men based upon evidence from a systematic literature review. The guideline, which was announced during the 2013 AUA Annual Meeting, recommends that men aged 55 to 69 years who are considering undergoing prostate cancer screening should talk with their physicians about the benefits and risks of screening.
Radium-223 dichloride (Xofigo) received FDA approval for the treatment of symptomatic metastatic castration-resistant prostate cancer that has metastasized to the bone but no other organs.
The majority of patients with systemic prostate cancer treated with androgen deprivation therapy (ADT) will develop castration-resistant prostate cancer (CRPC).

A 46-year-old man sought consultation for an abnormal prostate-specific antigen (PSA) level of 9 ng/mL and one prior negative biopsy. Five months ago, while traveling, he had presented to an urgent care facility with a 24-hour history of fever, chills, nausea, and vomiting.
A cohort-based study found that men with prostate cancer who took cholesterol-lowering statins had a lower risk of dying from their prostate cancer.

A case-control study of almost 500 men suggests that obese men who have had a benign prostate biopsy have a greater risk of prostate cancer in the future.

A mouse model of bone metastasis can be used to follow real-time response to therapeutics in preclinical development, such as cabozantinib, according to results presented in the poster session of the 2013 AACR annual meeting.
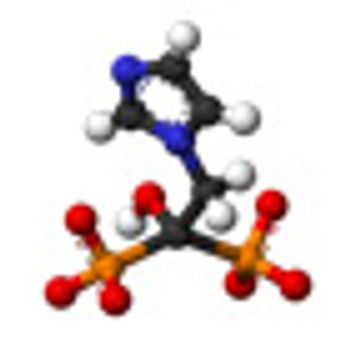
The use of zoledronic acid (Zometa) had no effect on the prevention of bone metastases in patients with high-risk prostate cancer, according to the first results of the Zometa European Study, or ZEUS, presented at the European Association of Urology 28th Annual Congress in Milan, Italy.

Researchers have identified the enzyme PKCζ, which acts as a tumor suppressor in prostate cancer and is part of a pathway that partly controls cell growth and metastasis.
The concept of multiparametric MRI comes at an important time in the history of prostate cancer screening. It is a method that provides anatomic information about the location, number, size, and risk of prostate cancers. It permits more accurate targeted biopsies that will improve the quality of tissue obtained, thereby reducing the rate of upstaging associated with random biopsies.
Multiparametric MRI is a promising tool for identifying cancer within the prostate. It has the potential to drastically change the way prostate cancer is staged and treated. However, work remains to make this technique reproducible and accessible to the community-based radiologist and urologist.

Only the possibility of increasing survival with better tumor localization and staging is probable with multiparametric MRI-and improved survival with MR imaging in prostate cancer has not been shown in a clinical trial or meta-analysis to date.

Our aims in this article are to describe the various imaging sequences that comprise the multiparametric MRI exam, as well as to review current literature on the strengths/weaknesses of these sequences; to delineate strategies for standardizing interpretation and reporting of MRI results; and to expound on the role of prostate MRI in clinical practice.

Targeting prostate cancer stem cells may be a method of treating prostate cancer while avoiding the development of resistance to androgen deprivation therapy, according to preclinical results presented at the annual meeting of the American Association for Cancer Research.
Advertisement
Advertisement
Trending on CancerNetwork
1
AI and MRD Take Center Stage on Day 2 of ASCO Breakthrough 2026
2
Sigvotatug Vedotin Does Not Significantly Improve Survival in NSCLC Trial
3
Cellular Therapy and Antibody-Drug Conjugates Shape Day 1 of ASCO Breakthrough 2026
4
GLP-1 Receptor Agonists Reduce Colorectal Cancer Risk in IBD Populations
5