














































































Further analyses of data subsets from the ALSYMPCA study of the alpha particle-emitting isotope Ra-223 (Xofigo) were presented at ASCO, providing additional evidence of efficacy and safety of the recently FDA approved therapeutic agent.
Genitourinary Cancers
Latest News
Advertisement
Advertisement
Addition of curcuminoids to treatment with docetaxel was well tolerated and showed promise in improving the response rate to docetaxel “in terms of both PSA decrease and objective response” in a phase II trial in patients with castration-resistant prostate cancer.
Monotherapy with enzalutamide (Xtandi) achieved a “high PSA response rate and marked PSA decline” in patients with hormone-naïve prostate cancer after 6 months in a single-arm, multicenter phase II study.
Treatment with 200 µmol per day of sulforaphane for 20 weeks was “feasible, safe,” and inhibited histone deacetylase (HDAC) function in a single-arm study of 20 patients who had non-castrate biochemical (PSA)-recurrence of prostate cancer despite surgery or radiation.

Ahead of the 2013 ASCO meeting we highlight some of this year's prostate cancer sessions, many of which focus on how best to use the new agents that have been approved recently, as well as looking into new drugs and combinations presented from early trials.

The use of cannabis among men has been linked to a significantly decreased risk for bladder cancer, according to a recent study; however, no cause and effect association has been found.

The AUA recently released its first set of treatment guidelines addressing the treatment of men with metastatic castration-resistant prostate cancer (mCRPC) at its 2013 Annual Meeting. The guidelines were released to address the increasingly complex treatment landscape available for patients with mCRPC.

Survival data of prostate cancer patients 70 and older show that those with three or more comorbidities and low- or intermediate-risk prostate cancer are less likely to die from prostate cancer than another health issue. But those with aggressive, high-risk disease are more likely to die from their prostate cancer.

Palliative radiotherapy is an effective means of alleviating pain and improving overall quality of life in elderly patients with bone metastases, according to a new study.
The American Urological Association (AUA) released a new clinical guideline detailing recommendations for the use of prostate cancer screening in average-risk men based upon evidence from a systematic literature review. The guideline, which was announced during the 2013 AUA Annual Meeting, recommends that men aged 55 to 69 years who are considering undergoing prostate cancer screening should talk with their physicians about the benefits and risks of screening.
Two genome-wide studies have identified a total of 12 new genetic loci associated with a higher risk of testicular cancer. The risk-associated genetic variations could help clinicians single out higher-risk men for screening and early detection.

The use of statins was independently associated with improvements in overall survival and disease-specific survival among a group of patients who had undergone partial or radical nephrectomy for renal cell carcinoma.
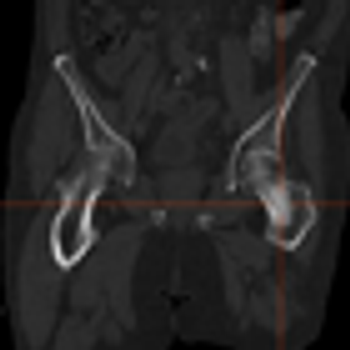
Radium-223 dichloride (Xofigo) received FDA approval for the treatment of symptomatic metastatic castration-resistant prostate cancer that has metastasized to the bone but no other organs.
The majority of patients with systemic prostate cancer treated with androgen deprivation therapy (ADT) will develop castration-resistant prostate cancer (CRPC).

A 46-year-old man sought consultation for an abnormal prostate-specific antigen (PSA) level of 9 ng/mL and one prior negative biopsy. Five months ago, while traveling, he had presented to an urgent care facility with a 24-hour history of fever, chills, nausea, and vomiting.
A cohort-based study found that men with prostate cancer who took cholesterol-lowering statins had a lower risk of dying from their prostate cancer.
A study found that robotic partial nephrectomy to remove kidney cancer tumors resulted in better outcomes, but also had significantly higher hospital charges. The data were presented at the annual meeting of the American Urological Association.

The FDA’s Oncologic Drugs Advisory Committee has voted 13 to 1 against AVEO's drug tivozanib for the treatment of patients with metastatic renal cell carcinoma.

A case-control study of almost 500 men suggests that obese men who have had a benign prostate biopsy have a greater risk of prostate cancer in the future.

A mouse model of bone metastasis can be used to follow real-time response to therapeutics in preclinical development, such as cabozantinib, according to results presented in the poster session of the 2013 AACR annual meeting.
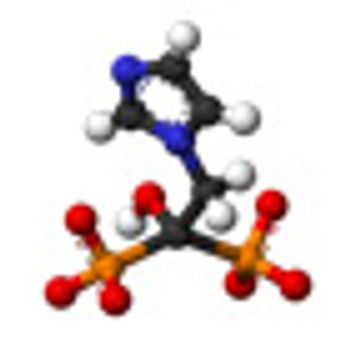
The use of zoledronic acid (Zometa) had no effect on the prevention of bone metastases in patients with high-risk prostate cancer, according to the first results of the Zometa European Study, or ZEUS, presented at the European Association of Urology 28th Annual Congress in Milan, Italy.

A new immunoassay that tests for the presence of nicotinamide N-methyltransferase (NNMT), L-plastin (LCP1), and nonmetastatic cells 1 protein (NM23A) may be an effective method for the early detection of malignant kidney cancer.

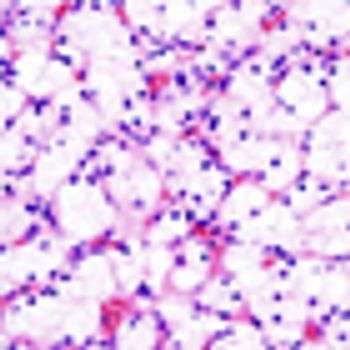
Even those renal cell carcinomas (RCCs) that are smaller than 4 cm may put patients at risk for aggressive cancer, according to a new study presented at the 28th Annual European Association of Urology Congress in Milan, Italy.

Researchers have identified the enzyme PKCζ, which acts as a tumor suppressor in prostate cancer and is part of a pathway that partly controls cell growth and metastasis.
The concept of multiparametric MRI comes at an important time in the history of prostate cancer screening. It is a method that provides anatomic information about the location, number, size, and risk of prostate cancers. It permits more accurate targeted biopsies that will improve the quality of tissue obtained, thereby reducing the rate of upstaging associated with random biopsies.
Advertisement
Advertisement
Trending on CancerNetwork
1
TOP Trial: Chemo-Osimertinib in TP53-Mutant EGFR-Mutated NSCLC
2
FLAURA2: Osimertinib Plus Chemo in EGFR-Mutant NSCLC
3
Access to Care and Drug Prices: Recent Department of Health and Human Services Guidance
4
Sequencing ADCs and Managing Ocular Toxicities in Breast Cancer Populations
5