















































































The accurate and in-depth documentation of learning gaps is a fundamental aspect of developing continuing education activities. To obtain a better understanding of community-based medical oncology practice patterns, 43 oncologists within the United States were recruited to complete a traditional clinical case–based questionnaire and to contribute specific anonymous demographic and treatment information derived from their actual patients. This information was used to create a cross-sectional case database on two types of cancer in which major clinical advances have been reported in recent years - multiple myeloma and follicular lymphoma. These diseases also are similar in that most patients experience clinically meaningful benefits from systemic treatment but are unlikely to be cured by therapy. As further described in this and the subsequent two articles, this case-based series documents that (a) clinical research advances are being quickly implemented in daily patient care and that (b) although therapeutic strategies vary based on patient age, the short-term outcomes in terms of response to and tolerance of treatment are similar in younger and older patients.
Hematologic Oncology
Latest News
A number of recent treatment advances in the management of follicular lymphoma (FL), including the introduction of the anti-CD20 monoclonal antibody rituximab, have effectively shifted the primary therapeutic goal away from palliation and avoidance of toxicity toward the more proactive objective of extending survival. This paper reviews recent practice patterns in the broad context of the published findings from major phase III randomized trials; it documents potential gaps between trial results and actual practice, and the implications of these for continuing education of oncologists. Forty-three US-based community oncologists participated in a cross-sectional case survey during which 40 documented their management of 186 patients with newly diagnosed FL and 133 patients with relapsed FL, all of whom were treated after January 1, 2008. The findings from this initiative indicate that the majority of these patients did not have any major symptoms at presentation. Additionally, tolerance of and response to treatment, regardless of the regimen employed, were similar across the different age groups studied (<65, 65-74, ≥75 years). Therapies selected by the physicians surveyed in both the up-front and the relapsed settings broadly corresponded to the evidence-based published literature and were supported by treatment guidelines. In addition, a change in the proportional use of bendamustine/rituximab (BR) in the up-front treatment of FL from 2008 to 2010 was observed, suggesting that community oncologists are rapidly incorporating pivotal clinical trial results when deciding on individual patient management strategies.
The management of multiple myeloma (MM) has undergone rapid change with the recent emergence of several effective novel agents that have added complexity to individualized treatment decision-making. This paper reviews the initial management of 276 patients with MM diagnosed and treated by 43 US-based community oncologists since January 1, 2008. The case survey data obtained are evaluated within the broad context of published findings from major phase III randomized trials and as such reveal potential education gaps and implications for oncology CME. Overall, the results reveal that most patients were symptomatic at diagnosis and were risk-stratified by fluorescene in situ hybridization (FISH) and/or cytogenetics. When analyzed by age, the overall symptomatology and biomarker-defined risk profiles appeared similar in the three age groups studied (
The effectiveness of RT in the palliative setting is sometimes overlooked; however, RT can provide excellent palliation for patients whose disease becomes refractory to other modalities.
Canadian researchers also find that patients are not having recommended cancer screening studies done on a regular basis.

Here we present the case of a 3-year-old girl with generalized lymphadenopathy and fever, in whom the cause of the symptoms was initially thought to be infectious. Ultimately, however, anaplastic large cell lymphoma (ALCL) was diagnosed. Using this case as a backdrop, we discuss the wide range of systemic illnesses that the differential diagnosis of generalized lymphadenopathy encompasses.
Combined with first-line chemotherapy, intravenous delivery therapy also confers a survival benefit over oral bisphosphonates. Gareth J. Morgan, MD, PhD, lead investigator of the Medical Research Council Myeloma IX study, will share additional trial results at ASH 2010.
Imatinib (Gleevec), the first-line standard of care in chronic myeloid leukemia, will become a generic drug in 2015, so the race is on to find a second generation of tyrosine kinase inhibitors (TKIs) that can do the job just as well.
Eighteen-month follow up supports lower-dose nilotinib as the new standard of care for newly diagnosed chronic myeloid leukemia. The ENESTnd trial (Evaluating Nilotinib Efficacy and Safety in Clinical Trials of Newly Diagnosed Ph+CML Patients) enrolled 846 patients at 217 sites in 35 countries. Timothy P. Hughes, MD, MBBS, will present an update to the ENESTnd trial at ASH 2010.
HIV’s disruption of immune system function may cause the immune system cells themselves to become cancerous, NCI researchers have concluded. If so, this might explain why patients with AIDS are 100 times more likely to be diagnosed with non-Hodgkin’s lymphoma than the general population.
This year's American Society of Clinical Oncology meeting featured a highly select lineup of sessions dealing with hematologic malignancies.
Standard therapy options are limited for patients with refractory chronic lymphocytic leukemia, with or without lymphadenopathy, and the results are generally poor. Ofatumumab (Arzerra), a novel human CD20 monoclonal antibody, could be the answer for improving outcomes in this patient population. Lead investigator William G. Wierda, MD, PhD, will share the final analysis of the results from this international study at ASH 2010.
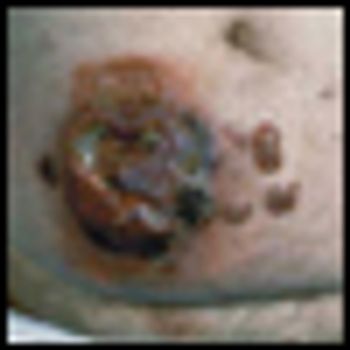
Anaplastic large cell lymphoma (ALCL) is a biologic and clinically heterogenous subtype of T-cell lymphoma. Clinically, ALCL may present as localized (primary) cutaneous disease or widespread systemic disease. These two forms of ALCL are distinct entities with different clinical and biologic features. Both types share similar histology, however, with cohesive sheets of large lymphoid cells expressing the Ki-1 (CD30) molecule. Primary cutaneous ALCL (C-ALCL) is part of the spectrum of CD30+ lymphoproliferative diseases of the skin including lymphomatoid papulosis. Using conservative measures, 5-year disease-free survival rates are>90%. The systemic ALCL type is an aggressive lymphoma that may secondarily involve the skin, in addition to other extranodal sites. Further, systemic ALCL may be divided based on the expression of anaplastic lymphoma kinase (ALK) protein, which is activated most frequently through the nonrandom t(2;5) chromosome translocation, causing the fusion of the nucleophosmin (NPM) gene located at 5q35 to 2p23 encoding the receptor tyrosine kinase ALK. Systemic ALK+ ALCLs have improved prognosis compared with ALK-negative ALCL, although both subtypes warrant treatment with polychemotherapy. Allogeneic and, to a lesser extent, autologous stem cell transplantation play a role in relapsed disease, while the benefit of upfront transplant is not clearly defined. Treatment options for relapsed patients include agents such as pralatrexate (Folotyn) and vinblastine. In addition, a multitude of novel therapeutics are being studied, including anti-CD30 antibodies, histone deacetylase inhibitors, immunomodulatory drugs, proteasome inhibitors, and inhibitors of ALK and its downstream signaling pathways. Continued clinical trial involvement by oncologists and patients is imperative to improve the outcomes for this malignancy.
Parents and their children need to understand that advancing science does not always go hand-in-hand with a direct benefit to the patients.
Mycosis fungoides (MF), the most common cutaneous T-cell lymphoma, is a low-grade cutaneous lymphoma characterized by skin-homing CD4+ T cells. It is notable for highly symptomatic progressive skin lesions, including patches, plaques, tumors, and erytheroderma, and has a poorer prognosis at later stages. Diagnosis remains difficult owing to MF’s nonspecific skin presentation and identification of the optimal treatment strategy is challenging given the paucity of controlled trials and numerous and emerging treatment options. Management includes topical therapy with the addition of systemic therapy for patients with later-stage disease including tumors; erythroderma; and nodal, visceral, or blood involvement. Topical therapies include mechlorethamine (nitrogen mustard), carmustine (BCNU), steroids, bexarotene gel (Targretin Gel), psoralen plus ultraviolet A (PUVA), ultraviolet B (UVB), and either localized or total skin electron radiotherapy. Systemic therapies include interferon, retinoids, oral bexarotene (Targretin), denileukin diftitox (Ontak), vorinostat (Zolinza), extracorporeal photochemotherapy (photopheresis), and cytotoxic chemotherapy. Herein, we outline clinically relevant aspects of MF, including clinical presentation, pathology, diagnosis, and staging. We describe in detail existing and emerging therapeutics and offer specific recommendations for management of each stage of MF.
The article entitled “Diagnosis and Management of Mycosis Fungoides” by Shira Galper, Benjamin Smith, and Lynn Wilson is an excellent contemporary summary of the workup and management of mycosis fungoides (MF) and its leukemia variant, Sézary syndrome (SS). In their discussion of the diagnosis and staging of MF and SS, the authors include a discussion of proposed revisions by the International Society for Cutaneous Lymphoma and the European Organisation for the Research and Treatment of Cancer (ISCL/EORTC) which seek to identify prognostic subgroups. In addition, there is a complete overview of the various treatment options for management of MF and SS. This treatment overview closely parallels the 2010 National Comprehensive Cancer Network (NCCN) Practice Guidelines for MF and SS.
Galper et al. should be commended for their concise and useful review of the diagnosis and management of mycosis fungoides (MF). It is notable that all of the authors are radiation oncologists. While the reader may expect a radiation oncologist’s perspective on the management of mycosis fungoides, their review goes beyond highlighting the various radiation techniques used in the treatment of MF. It highlights the major diagnostic dilemmas when evaluating patients with skin lesions that eventually are diagnosed as MF or its leukemic counterpart, Sézary syndrome (SS). It also stresses the importance of a multidisciplinary approach in diagnosing and caring for MF patients involving dermatology, dermatopathology, radiation oncology, and hematology/oncology, and provides a concise review of the treatment options in the MF and SS armamentarium. Navigating these options requires a good understanding of the natural history of the disease, the side effects of treatment, the expected response rates of treatment, the median time to response, the patient’s comorbid conditions, and goals of care.

With better disease definition, staging, and monitoring, treatment of extranodal NK/T-cell lymphoma is becoming more rational. A large proportion of patients with localized nasal disease may enjoy prolonged disease-free survival. On the other hand, early HSCT or novel therapy may be recommended for aggressive extranasal disease.
Dr. Bennett and colleagues have provided a thorough and balanced history of the rise and fall of erythropoietin-stimulating agents (ESAs) in cancer-associated anemia. Their review encourages us to think about the lessons learned from this history-lessons about medical progress, the importance of clinical research in guiding clinical practice, and the role of the US Food and Drug Administration (FDA) in protecting patients
The perception and reality of the clinical value of erythropoiesis-stimulating agents (ESAs) in cancer supportive care have undergone a dramatic transformation since their initial use in 1990. The perception of ESA value in patients has evolved from panacea to miscreant over a 2-decade period of laboratory research, clinical trial data, and postmarketing experience. Meanwhile, the real clinical benefits of ESAs have changed very little from those described in the joint American Society of Clinical Oncology/American Society of Hematology guidelines originally published in 2002.[1] Even then, the value of initiation of ESAs was clear only in patients with hemoglobin values < 10 g/dL; quality-of-life measures produced inconsistent and, therefore, clinically inapplicable, results; and ESA use was shown to reduce the proportion of patients requiring red blood cell (RBC) transfusions by approximately 20%. The reality of ESA use that came to light following approval was increased mortality rates in certain populations, higher tumor progression and cancer recurrence rates, and more frequent and severe serious adverse effects including thromboembolism, stroke, and cardiovascular events.
Multiple myeloma remains the second most common hematologic malignancy in the United States, after non-Hodgkin lymphoma.
Anemia is a widely prevalent complication among cancer patients. At the time of diagnosis, 30% to 40% of patients with non-Hodgkin lymphoma or Hodgkin lymphoma and up to 70% of patients with multiple myeloma are anemic; rates are higher among persons with myelodysplastic syndromes. Among patients with solid cancers or lymphomas, up to half develop anemia following chemotherapy. For almost 2 decades, erythropoiesis-stimulating agents (ESAs) were the primary treatment for cancer-related anemia. However, reassessments of benefits and risks of ESAs for cancer-associated anemia have occurred internationally. We reviewed guidelines and notifications from regulatory agencies and manufacturers, reimbursement policies, and utilization for ESAs in the cancer and chronic kidney disease settings within the United States, Europe, and Canada. In 2008 the US Food and Drug Administration (FDA) restricted ESAs from cancer patients seeking cure. Reimbursement is limited to hemoglobin levels < 10 g/dL. In the United States, ESA usage increased 340% between 2001 and 2006, and decreased 60% since 2007. The European Medicines Agency (EMEA) recommended that ESA benefits do not outweigh risks. In Europe between 2001 and 2006, ESA use increased 51%; since 2006, use decreased by 10%. In 2009, Canadian manufacturers recommended usage based on patient preferences. In Canada in 2007, approximately 20% of anemic cancer patients received ESAs, a 20% increase since 2004. In contrast to Europe, where ESA use has increased over time, reassessments of ESA-associated safety concerns in the United States have resulted in marked decrements in ESA use among cancer patients.
Hematopoietic malignancies account for 6% to 8% of new cancers diagnosed annually. In the year 2009, an estimated 44,790 new cases of leukemia were diagnosed, and 21,870 deaths were attributable to leukemias of all types. The total age-adjusted incidence of leukemia, including both acute and chronic forms, is 9.6 per 100,000 population; the incidence of acute lymphoblastic leukemia (ALL) is 1.5 per 100,000 and of acute myelogenous leukemia (AML) is 2.7 per 100,000 population.
The incidence rates of non-Hodgkin lymphoma (NHL) in the United States have almost doubled between 1970 and 1990, representing one of the largest increases of any cancer. Although the overall incidence rates of NHL began to stabilize in the late 1990s, the temporal trends varied by histologic subtype. Some of this increase may be artifactual, resulting from improved diagnostic techniques and access to medical care, or directly related to the development of NHL in 25- to 54-year-old men with human immunodeficiency virus (HIV) infection. However, additional factors must be responsible for this unexpected increase in frequency of NHL that has been observed throughout the United States.
In 2009 approximately 8,510 new cases of Hodgkin lymphoma (HL) will be diagnosed in the United States. Over the past 4 decades, advances in radiation therapy and the advent of combination chemotherapy have tripled the cure rate of patients with HL. In 2009, more than 80% of all newly diagnosed patients can expect a normal, disease-free life span.