















































































The number of patients in the U.S. treated with radiation has increased at an average annual rate of about 7% between 2007 and 2009, according to the “2010 Radiation Therapy Market Summary Report” by IMV. Breast, prostate, and lung cancers continue to be the cancer types treated most frequently with radiation.
Lung Cancer
Latest News

Advertisement
Advertisement
Patients with advanced non-small-cell lung cancer achieved a significant increase in survival time when tumor treating fields (TTF) therapy was added to their chemotherapy. In a single-arm, phase II study, physicians delivered TTF therapy, using the NovoTTF-100L from Novocure, to 42 patients with stage IIIb-IV metastatic NSCLC who had failed prior treatments. Patients in the study received TTF therapy for 12 hours a day in combination with pemetrexed (Alimta) every three weeks until disease progression.

Finding an effective treatment for all the complex iterations of cancer is akin to chasing an outlaw through a treacherous mountain range, in the estimation of Louis M. Weiner, MD, director of the Georgetown Lombardi Comprehensive Cancer Center in Washington, DC.

Research from Japan documenting remarkable survival rates among patients with inoperable lung cancer may only hint at the potential of proton-beam radiation therapy. The study out of the Proton Medical Research Center in Tennoudai, Japan, documented high survival rates for 55 patients suffering from stage I inoperable non-small-cell lung cancer.
Novartis and its partner Antisoma announced that an interim analysis of data from a late-stage trial showed that vadimezam (ASA404) was unlikely to provide any benefit as a second-line treatment for patients with non-small-cell lung cancer. As a result, Novartis indicated that it would halt development of the compound, which was designed to inhibit angiogenesis.

The key to effective treatment of squamous lung cell lung cancer in smokers may be at hand.

Patients with incurable NSCLC are less likely to progress to second-linetherapy with the right maintenance regimen. But maintenance therapyalso means committing patients to continuous treatment without anybreaks or chances to recover from adverse events.
With the new direction in research and clinical trials, treating patients who most benefit from treatment with minimal toxicity will continue to be the mainstay of personalized cancer therapy.
Bevacizumab has become a standard of care for first line therapy in a subgroup of advanced NSCLC patients. With the advent of other effective therapies in bevacizumab-eligible patients and the ongoing development and testing of biomarkers for cytotoxic agents, it remains to be seen whether continued use of bevacizumab will be justified in the absence of predictive biomarkers.
Despite the fact that bevacizumab and cetuximab are both in an advanced stage of clinical development for use in treatment for unresectable NSCLC (with bevacizumab already licensed for the use in clinical practice), several unanswered questions regarding these drugs remain. A number of ongoing trials have been specifically addressed to answer them, however, the first priority should be to personalize treatment, through clinical or biological markers, in order to better select patients who could benefit from targeted therapy with decreased toxicity.

The search for a magic bullet against cancer historically has glowed bright then dimmed, depending on the stage of discovery. Developments surrounding monoclonal antibodies and angiogenesis inhibitors have followed this cycle, as exuberance for their potential has bowed to the nuances that underlie the complex mechanisms on which they depend.
Despite the fact that elderly patients comprise over 50% of the non-small cell lung cancer (NSCLC) population, our knowledge regarding the efficacy and safety of chemotherapy in this group is suboptimal. The “elderly” (defined as individuals ≥70 years of age) experience physiologically normal aging of their bone marrow and kidneys, which inherently increases toxicity to therapy. Standard practice has often been to discourage the use of combination chemotherapy in these patients; however, general consensus guidelines emphasize that performance status should primarily guide the choice of treatment. Elderly patients with advanced NSCLC treated with platinum doublet therapy demonstrate similar efficacy (but increased toxicity) to their younger counterparts. Patients with metastatic disease in which a targeted and/or biological agent(s) was added to chemotherapy experienced benefits similar to those treated with standard platinum doublets, but with increased morbidity and mortality. In the future, effective testing of molecular targeted therapies will have to include elderly patients among research cohorts or risk excluding a large population of eligible patients. Overall, elderly patients with advanced NSCLC, while experiencing greater toxicity, demonstrate the same response rates and survival benefits as their younger peers.
Calendar age and biological age do not always correspond. Pablo Picasso, source of the quote that begins the title of this commentary, lived a notoriously robust and active life through his later decades, dying in his nineties in the midst of a dinner party. In the oncology community, with the advent of targeted therapeutics and better supportive care, the disparity between the two is likely to be increasingly relevant to both research and practice. In this issue of ONCOLOGY, Chiappori et al review data supporting the idea that even in the context of standard cytotoxic chemotherapy, elderly patients with advanced NSCLC experience similar response rates and similar survival benefits to those seen in younger patients. They note that biases excluding elderly patients from clinical trials result in gaps in our knowledge of how to best treat older patients.
The review by Dr. Chiappori and colleagues in this issue of ONCOLOGY addresses an important challenge relating to the optimal management of elderly patients with lung cancer. The authors provide an excellent overview of the data in patients with various stages of non-small cell lung cancer (NSCLC). They also highlight the limitations of the existing data in the management of elderly NSCLC patients.
All trials are not equal, even those conducted by the NCI. It’s all about design, according to leading lung cancer specialist.
20% fewer lung cancer deaths seen among those who were screened with low-dose spiral CT than with chest X-ray
Research from Japan documenting remarkable survival rates among patients with inoperable lung cancer may only hint at the potential of proton beam therapy.
In these patients with substantial symptoms and short life expectancy, there's no reason to delay delivery of palliative care.
Ganti and colleagues have provided a brief review on the diagnosis of small-cell lung cancer (SCLC) and the roles of chemotherapy and surgery in its management. Notably, in the past three decades, the most significant progress in the treatment of SCLC has mainly involved the use of radiotherapy. Thus, to complement their assessment, we will provide an overview of the role of radiation in the management of limited-stage and extensive-stage SCLC.
Small-cell lung cancer (SCLC) is a pathologically distinct malignancy of the lung, characterized by rapid growth, propensity for early metastatic spread, and responsiveness to chemotherapy and radiation. Despite its generally good initial response, the relapse and subsequent mortality rate remain very high. Only 3% to 8% of all patients survive 5 years, and median survival for extensive stage disease is 8 to 13 months.[1,2]
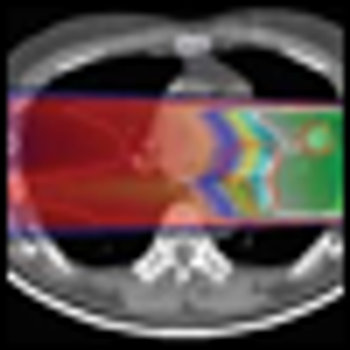
The role of radiation therapy (RT) in lung cancer is long established; some of the earliest Radiation Therapy Oncology Group reports dealt with non-small cell lung cancer (NSCLC).[1,2] More recently, the advent of stereotactic body RT (SBRT) techniques has provided significant local control rates after focused treatment of selected small metastases and inoperable early stage lesions.[3,4] Our center has been in the forefront of examining SBRT and its role in central [5] or bilateral [6] lesions, its effect on PET imaging [7] and pulmonary function testing,[8] and subsequent frequency of brachial plexopathy,[9] chest wall toxicity,[10] or pneumonitis.[11] Still, even this highly conformal technique comes with potentially significant dose to adjacent normal tissue. This is in the context of an emerging appreciation for the pulmonary consequences of elevated mean lung dose,[12] or V5 after pneumonectomy.[13] For each lung cancer patient requiring RT, an effective mechanism to deliver dose to the tumor while minimizing dose to uninvolved lung is called for. Enter protons.
In the conclusion to the article “Proton Radiation Therapy for Lung Cancer: Is There Enough Evidence?” Dr. David Bush puts his finger on the critical issue underlying most debates about the value of new medical technologies. He notes that “The evidence required to bring new technology into clinical practice is poorly defined.”[1] In the specific context of this article, the answer to the question of whether or not there is enough evidence depends entirely on how one chooses to define “enough.” Some experts believe that biological modeling based on dose distributions is sufficient to conclude that proton therapy improves health outcomes. Others have argued that the evidence is only adequate once randomized clinical trials have been completed to directly compare alternative interventions. Whatever one’s position on this issue, the lack of clarity on the question of adequacy of evidence is a major contributor to the gaps in knowledge about the comparative effectiveness of many widely used clinical interventions. Accelerating the rate at which this knowledge is generated will require a serious and sustained effort to define these evidence thresholds. This would allow more energy to be channeled into generating the needed evidence and less energy to be devoted to debating whether or not the evidence we have today is good enough.
Just as in recent years attitudes and treatment therapies have changed regarding non–small-cell lung cancer (NSCLC), it is time that the same occur for its small-cell counterpart. Although treatment for advanced-stage small-cell lung cancer (SCLC) is fairly standardized, there remain a number of controversies that have yet to be clarified by evidence-based data.
Proton radiation for cancer offers the ability to conform the high-dose region of radiation therapy to the tumor while reducing the dose of radiation to adjacent normal tissues. In lung cancer, this equates to greater sparing of uninvolved lung, heart, esophagus, and spinal cord. Sparing these normal tissues permits the delivery of higher-radiation doses to the tumor. Studies that compare the distribution of radiation doses for lung cancer show that proton radiation is superior, even when factors such as respiratory motion are considered. Clinical experience confirms the feasibility of proton radiation for early-stage non-small-cell lung cancers, and clinical trials are being conducted in locally advanced tumors: To date, evidence indicates that proton radiation should be further explored.
Despite a decreasing incidence in the United States, small-cell lung cancer (SCLC) remains a major clinical problem, with approximately 30,000 new cases each year. The diagnosis of SCLC is usually not difficult. The Veterans Administration Lung Study Group (VALSG) staging system is less accurate than the American Joint Committee of Cancer tumor-node-metastasis (TNM) system (7th edition) at predicting survival in SCLC, especially in lower stage disease. Surgery has not played a major part in the management of SCLC, but emerging data suggest that resection may have a role in earlier stage disease. While the frontline treatment of SCLC has not changed significantly in the past decade, newer agents that are currently being investigated provide hope for better treatment of relapsed/refractory disease for the future.
Advertisement
Advertisement
Trending on CancerNetwork
1
Sacituzumab Govitecan Receives FDA Approval Across 2 TNBC Indications
2
Where Does LAG-3/PD-1 Inhibition Fit In PD-1–Refractory Hodgkin Lymphoma?
3
VS-7375 Exhibits Activity in KRAS G12D–Mutated Solid Tumors
4
GLP-1 Receptor Agonists Reduce Colorectal Cancer Risk in IBD Populations
5