




















































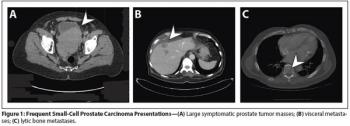
Aggressive variants of prostate cancer often take the form of neuroendocrine or small-cell carcinomas, which frequently lack androgen receptor expression and respond poorly to hormonal therapies.
Aggressive variants of prostate cancer often take the form of neuroendocrine or small-cell carcinomas, which frequently lack androgen receptor expression and respond poorly to hormonal therapies.
In spite of recent encouraging developments in the setting of GI neuroendocrine tumors, many clinical questions remain to be answered and will be highlighted in this commentary.
The relative abundance of new data on the biological underpinnings of neuroendocrine tumors, combined with clinical trial data supporting new treatment options, is a clear sign of progress. Yet, as is so often the case, these recent studies have generated a multitude of new and different questions.
In this review, we summarize biologic, pathologic, and clinical aspects of gastroenteropancreatic-neuroendocrine tumors, focusing on recent advances in their treatment.
Researchers used an unbiased bioinformatics approach to identify a class of drugs currently used for non-cancer treatment that could be used to treat small-cell lung cancer, a cancer type for which there are few treatment options.

A combined dual inhibition of vascular endothelial growth factor (VEGF) and c-MET is showing promise in preventing tumor invasion and metastasis. The data thus far are in a laboratory model of pancreatic neuroendocrine cancer.
Inherited mutations in the ataxia telangiectasia mutated (ATM) gene increase the odds of developing pancreatic cancer according to a new study. While there is predisposition for pancreatic cancer with up to 10% of cases occurring among families with a history of the disease, the genetic basis for this had not been previously discovered.
The review of surgical management of neuroendocrine tumors (NETs) of the gastrointestinal tract, authored by Huang, Poultsides, and Norton, is both comprehensive and accessible for readers of all backgrounds.
This article reviews the surgical management of gastrointestinal neuroendocrine tumors, including the preoperative control of hormonal symptoms, extent of resection required, postoperative outcomes, and differing management strategies as determined by whether the tumor has arisen sporadically or as part of a familial disorder, such as multiple endocrine neoplasia type 1.
Tumors of neuroendocrine origin arising from the pancreas, luminal gastrointestinal tract, and other tissues differ greatly in their malignant potential.
Data published in the Journal of Clinical Oncology show that patients with advanced neuroendocrine tumors (NET) of the midgut who were treated with octreotide acetate (Sandostatin LAR Depot) experienced a 66% reduction in risk of disease progression vs placebo.
One hundred years after Oberndorfer coined the word “carcinoid,” neuroendocrine tumors (NETs) are thought to be rare tumors characterized by the capacity for hormone production and often an indolent course. Recent data from population-based registries have shown a significant rise in the diagnosed incidence of NETs over the past 3 decades.
Metastatic well or moderately differentiated neuroendocrine tumors of the gastrointestinal tract and lung (NETs) are a fascinating and markedly heterogeneous group of generally indolent, but relentless cancers.
The patient is a 39-year-old Caucasian male who presented with a right renal mass and painless gross hematuria. He underwent a right laparoscopic radical nephrectomy and the final pathology revealed a carcinoid tumor.
Primary neuroendocrine neoplasms of the lung represent a clinical spectrum of tumors ranging from the relatively benign and slow-growing typical carcinoid to the highly aggressive small-cell lung carcinoma. The rarity of carcinoids has made the role of radiation therapy in their management controversial. This review considers the results of published studies to generate treatment recommendations and identify areas for future research. Surgery remains the standard of care for medically operable disease. Histology plays the most important role in determining the role of adjuvant radiation. Resected typical carcinoids likely do not require adjuvant therapy irrespective of nodal status. Resected atypical carcinoids and large-cell neuroendocrine carcinomas have a significant risk of local failure, for which adjuvant radiation likely improves local control. Definitive radiation is warranted in unresectable disease. Palliative radiation for symptomatic lesions has demonstrated efficacy for all histologies. Collaborative group trials are warranted.
Primary neuroendocrine neoplasms of the lung represent a clinical spectrum of tumors ranging from the relatively benign and slow-growing typical carcinoid to the highly aggressive small-cell lung carcinoma. The rarity of carcinoids has made the role of radiation therapy in their management controversial. This review considers the results of published studies to generate treatment recommendations and identify areas for future research. Surgery remains the standard of care for medically operable disease. Histology plays the most important role in determining the role of adjuvant radiation. Resected typical carcinoids likely do not require adjuvant therapy irrespective of nodal status. Resected atypical carcinoids and large-cell neuroendocrine carcinomas have a significant risk of local failure, for which adjuvant radiation likely improves local control. Definitive radiation is warranted in unresectable disease. Palliative radiation for symptomatic lesions has demonstrated efficacy for all histologies. Collaborative group trials are warranted.
Primary neuroendocrine neoplasms of the lung represent a clinical spectrum of tumors ranging from the relatively benign and slow-growing typical carcinoid to the highly aggressive small-cell lung carcinoma. The rarity of carcinoids has made the role of radiation therapy in their management controversial. This review considers the results of published studies to generate treatment recommendations and identify areas for future research. Surgery remains the standard of care for medically operable disease. Histology plays the most important role in determining the role of adjuvant radiation. Resected typical carcinoids likely do not require adjuvant therapy irrespective of nodal status. Resected atypical carcinoids and large-cell neuroendocrine carcinomas have a significant risk of local failure, for which adjuvant radiation likely improves local control. Definitive radiation is warranted in unresectable disease. Palliative radiation for symptomatic lesions has demonstrated efficacy for all histologies. Collaborative group trials are warranted.
Malignant small bowel tumors are extremely rare, accounting for 0.1% to 0.3% of all malignancies. Fewer than 2,400 new cases of small bowel malignancy are reported in the United States each year.[1] Malignant tumors, which account for about two-thirds of all primary small bowel tumors, consist of four primary subtypes: adenocarcinoma, carcinoid tumor, lymphoma, and sarcoma (or gastrointestinal [GI] stromal tumor). Each malignancy is characterized by unique predisposing factors, anatomy, and biology. The prevalence, pattern, and relevance of both regional lymph node and distant metastases differ. As a result, the study of malignant small bowel tumors, taken as an aggregate, is fraught with difficulty.