





















































Cancer survivors are at an increased risk for developing a second smoking-associated cancer if they smoked cigarettes prior to their first cancer diagnosis.
Cancer survivors are at an increased risk for developing a second smoking-associated cancer if they smoked cigarettes prior to their first cancer diagnosis.
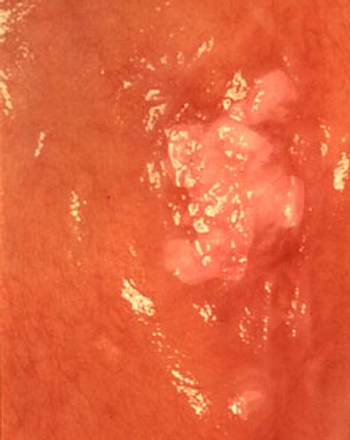
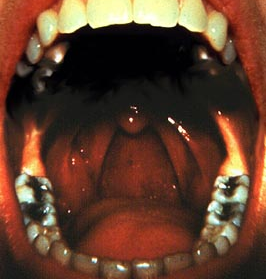
Using tobacco is linked to an increased risk of infection with oral HPV type 16, a sexually transmitted virus known to cause cancers of the mouth and throat.
In patients with recurrent or metastatic head and neck squamous cell carcinoma, afatinib better delayed cancer progression compared with methotrexate, according to results presented at the 2014 ESMO Congress.
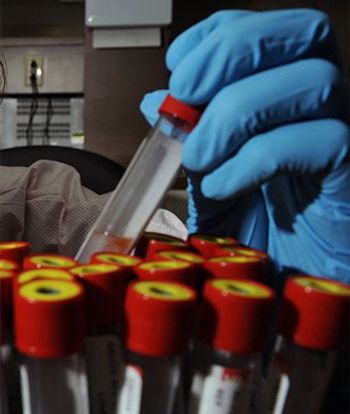
Researchers have developed a preliminary test using blood and saliva samples to detect disease recurrence in patients with HPV-related head and neck cancer.

A 74-year-old man presented with a 2.5-cm ulcerated mass occupying the middle third of his left outer ear, approximating the helical rim.
A phase II study demonstrated that cetuximab plus docetaxel-based chemoradiotherapy postoperatively in patients with high-risk squamous cell carcinoma of the head and neck led to improved disease-free and overall survival.
High-risk HPVs may be present more frequently than previously estimated in a variety of head and neck cancers, supporting the use of a combination of methods to detect high-risk strains.
A small retrospective study has identified several biomarkers that were significantly altered in patients with head and neck squamous cell carcinoma. If further validated, these serum biomarkers could facilitate early diagnosis.
Researchers have identified several risk factors that may help predict which patients with oropharyngeal cancer may require a percutaneous endoscopic gastrostomy tube during chemoradiotherapy, according to a newly published review.
Black race did not adversely affect outcomes after receiving radiotherapy for head and neck squamous cell carcinoma compared with white race, according to the results of a study in which black patients made up the majority of enrolled participants.
A new study of the relationship between BRAF V600E mutation status and its effect on papillary thyroid carcinoma found a negative association with clinicopathologic features suggestive of more aggressive disease.
The use of altered fractionation radiotherapy increased overall survival in patients with locally advanced head and neck cancers when compared with standard radiation, according to the results of a meta-analysis presented on Saturday at the 2013 European Cancer Congress in Amsterdam.
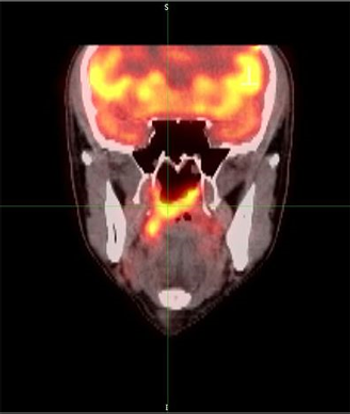
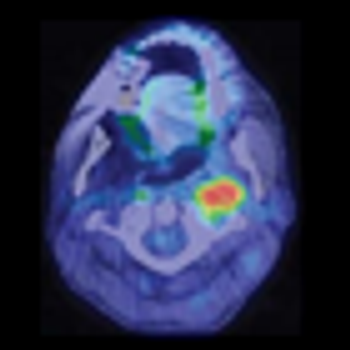
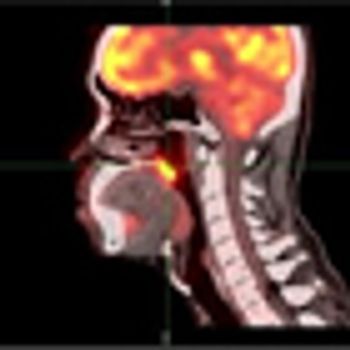
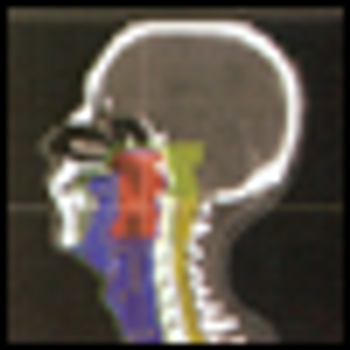
Researchers in China have found that the use of [18F] fluorodeoxyglucose PET/CT detected a greater number of distant metastases than conventional work-up imaging in patients with nasopharyngeal carcinoma.
Researchers in Canada have shown for the first time that the incidence of HPV-related oropharyngeal cancers is increasing among the Canadian population.
Neck dissection may no longer be the only surgical option for pathologic staging of the neck in patients with oral cavity squamous cell carcinoma, according to a new study.
More than one-third of patients with oropharyngeal cancer were seropositive for HPV16 E6 an average of 6 years prior to their cancer diagnosis compared with less than 1% of healthy controls, a new study has found.
Researchers have developed and tested a nomogram that uses various factors and can predict risk of recurrence in patients with major salivary gland carcinoma.
Prophylactic use of the SSRI escitalopram decreased the occurrence of depression in patients with head and neck cancers by 50% and resulted in significantly improved quality of life for 3 months after drug cessation, according to the results of the PROTECT trial.

A new population-based study of never-smokers shows those with gastric reflux are more likely to be diagnosed with cancers of the throat, including the voice box.
Locoregional recurrences are a major source of morbidity and mortality for patients with squamous cell carcinomas of the head and neck (HNSCC).
Two-year results from the largest randomized trial of IMRT in head and neck cancer confirm that it dramatically reduces the risk of dysphagia and xerostomia. The study was too small to establish a survival advantage, although the results are encouraging.
This paper by Drs. Bhayani, Holsinger, and Lai describes a new approach to an old problem. Advances in the management of head and neck cancer over the past few decades have been made predominantly in the area of non-surgical therapy. Starting with the Veterans Affairs Cooperative Trial for laryngeal cancer in the early 1990’s,[1] advances in the administration of chemotherapy and radiation therapy have enabled patients to forego traditional extensive resections that compromised speech and swallowing function.[2] The advances in combined chemoradiation for advanced head and neck cancer have come with a detriment to some patients in survival and quality of life.[3] Effective treatment, but with decreased morbidity was needed.
A series of promising new advances have emerged in H&N oncology in recent years. Among these are the advancement of highly conformal radiation delivery techniques (e.g. IMRT, protons); the successful introduction of molecular targeted therapies (e.g. cetuximab); the recognition of HPV as a powerful prognostic biomarker; and the development of minimally invasive surgical techniques. The application of transoral robotic surgery (TORS) in H&N cancer is reviewed by Bhayani et al in this issue of ONCOLOGY[1].
The article presented by Bhayani, Holsinger, and Lai thoroughly evaluates the emergence of transoral robotic surgery (TORS) as a technique in the field of otolaryngology. Transoral approaches to the upper aerodigestive tract, whether for diagnostic or therapeutic purposes, represent core tenets of the discipline and formed one of the bases for the inception of the specialty. Innovations and refinements in optics and materials have steadily increased the view, reach, and, consequently the effectiveness of the endoscopic surgeon with each passing decade. In the past thirty years, the introduction of the laser has further enhanced the capabilities of the surgeon, augmenting treatment options beyond open tumor resection and chemoradiation. The introduction of the daVinci robot is an incremental step in the development of techniques that have been evolving over the past one hundred and twenty years.
The evolution of surgical oncologic technology has moved toward reducing patient morbidity without compromising oncologic resection. In head and neck surgery, organ-preserving techniques have paved the way for the development of transoral techniques that remove tumors of the upper aerodigestive tract without external incisions and potentially spare the patient adjuvant treatment. The introduction of transoral robotic surgery (TORS) improves upon current transoral techniques to the oropharynx and supraglottis. This review will report on the evolution of robotic-assisted surgery: We will cover its applications in head and neck surgery by examining early oncologic and functional outcomes, training of surgeons, costs, and future directions.