















































































The liquid biopsy test is approved to identify patients who may benefit from treatment with specific FDA-approved targeted therapies.
The liquid biopsy test is approved to identify patients who may benefit from treatment with specific FDA-approved targeted therapies.

Though further research is necessary, researchers suggested that immune checkpoint inhibitors can be used as an individualized therapy in certain patients who have undergone solid organ transplantation.

A restrospective study published in JAMA Dermatology found that integrating dermatologic care into oncology practices might be associated with an increased adherence to evidence-based prophylaxis for EGFRi-associated rash.

The FDA approved the FoundationOne Liquid CDx based on analytical and clinical validation studies that included more than 7500 samples and 30,000 unique variants across over 30 cancer types.

The recommendations were developed on the basis of the ESMO Scale for Clinical Actionability of molecular Targets (ESCAT) ranking for genomic alterations occurring in the 8 cancers responsible for the most deaths worldwide.
These study findings suggest that the response rate to immune checkpoint blockade may be dependent on the strength of immune selection occurring early in tumorigenesis.
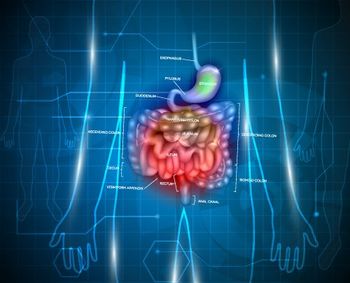
Bristol Myers Squibb announced that their phase 3 CheckMate-649 trial demonstrated superior overall survival and profession-free survival using nivolumab plus chemotherapy to treat patients with gastric and esophageal cancers.
The FDA approved Guardant360 CDx, the first liquid biopsy companion diagnostic that also uses next-generation sequencing technology to identify patients with any solid malignant neoplasm.

The oncologist from the Morrison Cancer Center explained why he believes the general population should not receive multi-gene panel testing.
The goal of the initiative is to have cancer screenings that were made in the first half of 2020 and cancelled due to COVID-19 rescheduled to ensure patients are again receiving routine screenings.
These findings have serious implications for future cancer care and underscore the need to resume cancer care and screening.
The National Comprehensive Cancer Network published a document intended for patients to understand how CAR-T cells work and what side effects are associated with the treatment.

The director of Molecular Pathology and assistant professor of Pathology at Cedars-Sinai spoke about the use of NGS testing to match patients with targeted therapy.
Adjuvant immunotherapy induced improved survival compared with those who did not in patients with stage 3 melanoma, according to data from a large real-world database.
RO7198457 in combination with atezolizumab induced significant levels of neoantigen-specific immune responses with a manageable safety profile in patients with locally advanced or metastatic solid tumors.

The expert from the American Cancer Society spoke about updated guidelines published recently regarding recommendations on diet and physical activity for cancer prevention.
The FDA approved pembrolizumab for the treatment of adult and pediatric patients with unresectable or metastatic tumor mutational burden-high solid tumors.
Experts discuss the case of a 56-year-old white man who presents with multiple immune-related adverse events
A clinically applicable mathematical model was developed by researchers to predict outcomes to immunotherapy for patients with cancer previously treated with anti–CTLA-4 or anti–PD-1/PD-L1 antibodies.
Interim data from cohort B of KEYNOTE-555, a phase I trial evaluating a 400 mg every 6-week dosing regimen of pembrolizumab in patients with metastatic melanoma, demonstrated a consistent benefit-risk profile.

The FDA approved an additional recommended dose of 400 mg pembrolizumab (Keytruda) every 6 weeks across all adult indications.

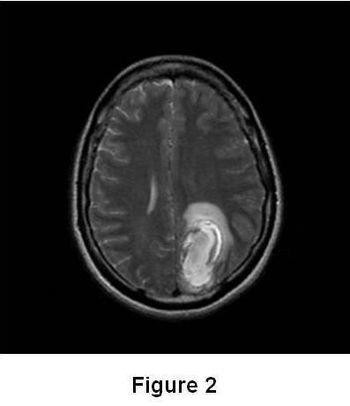
The study found that pembrolizumab has activity in brain metastases from non-small cell lung cancer that is similar to its systemic activity and can result in prolonged survival in a subset of patients.
A recent study determined 4 distinct long noncoding RNA-based immune classes for patients with cancer and provided scores for integration into multiomic panels for precision immunotherapy.
Researchers found that the potential availability of CAR T-cell therapies for large B-cell lymphomas with lower adverse event rates that are suitable for outpatient administration may reduce the total costs of care.

The FDA cleared the investigational new drug (IND) application for the use of CYNK-001 in adults with COVID-19.