
María Teresa Bourlon, MD, MSc, FASCO, discussed why early RadiCal trial closure and adverse effects outweigh secondary survival signals in bone-metastatic RCC.
María Teresa Bourlon, MD, MSc, FASCO, discussed why early RadiCal trial closure and adverse effects outweigh secondary survival signals in bone-metastatic RCC.

María Teresa Bourlon, MD, MSc, FASCO, discussed data showing body composition and muscle loss with lenvatinib/everolimus vs cabozantinib in metastatic ccRCC.

This cross-sectional study evaluated the genetic landscape of a cohort of patients with metastatic prostate cancer who were treated at a referral center in Mexico City, Mexico.

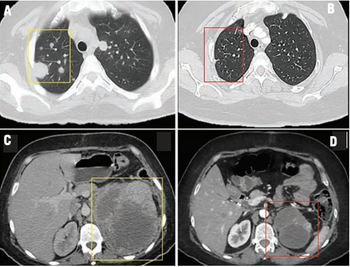
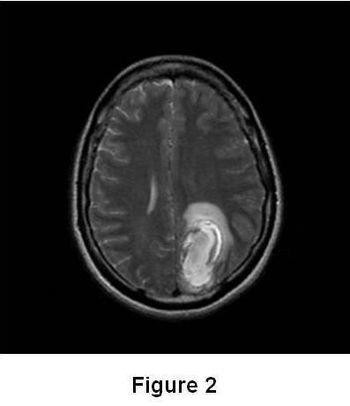
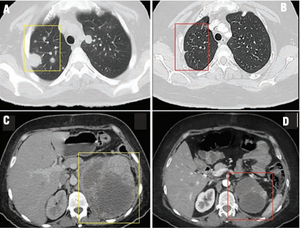
A 47-year-old woman with a history of drug-resistant epilepsy during childhood presented to the emergency department with sudden dyspnea and chest pain. Upon admission, her oxygen saturation was 88%.
Francisco Castro-Alonso, MD, and colleagues describe the effects of the use of erdafitinib in a patient with metastatic urothelial bladder cancer.
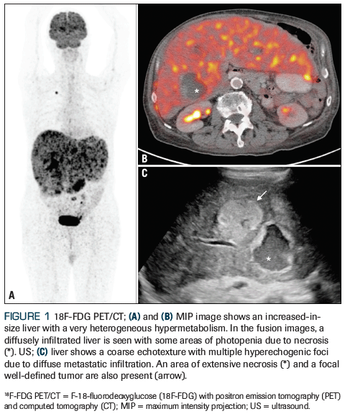
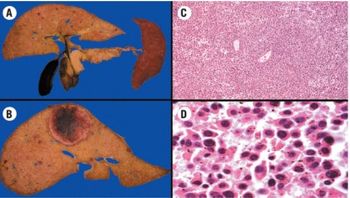
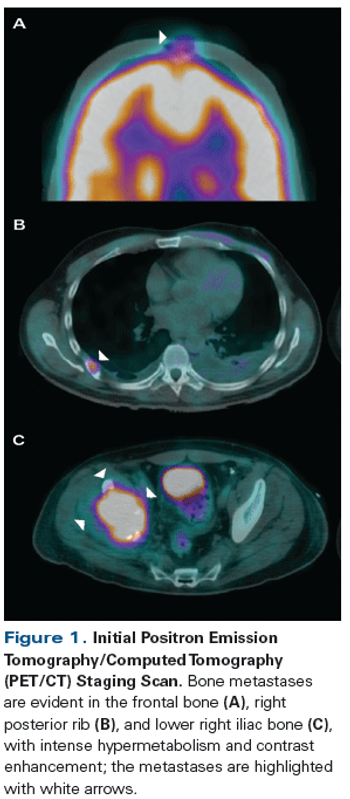
In this installement of Clinical Quandaries, Abigail Mateos-Soria, MD, and colleagues present a case of an 38-year-old woman who has a 3-month history of fatigue, dyspnea, significant weight loss, and severe left flank pain.
In this edition of Clinical Quandaries, Regina Barragan-Carrillo, MD, and colleagues present a case of an 18-year-old man who has a 1-month history of nonpainful right testicular enlargement.
This clinical quandary details a Mexican man, aged 77 years, who presented to the oncology clinic with a sternal mass. Based on the results, the patient fulfilled the 2016 American College of Rheumatology/European League Against Rheumatism classification criteria for Sjögren syndrome, thus the diagnosis triggered by immune checkpoint inhibitors was definitively established.

Another installment of Clinical Quandaries is presented by Karen Férez-Blando, MD, and colleagues of a 45-year-old man with a diagnosis of intermediate-risk stage IV clear cell renal carcinoma who develops grade 2 hand-foot skin reaction on sunitinib therapy.

Key points: Patients with disorders of sex development (DSDs) are at an increased risk of malignant germ cell tumors (GCTs). In adulthood, the partial form of androgen insensitivity syndrome confers the greatest risk of developing malignant GCTs. Gonadoblastoma is the most common gonadal GCT arising in patients with DSDs. Despite being a benign neoplasm, it can undergo malignant transformation in up to 60% of patients with a DSD. Oncologic treatment in patients with disorders of sex development and malignant GCTs does not differ from the standard treatment for testicular GCTs. Treatment of patients with DSDs requires a multidisciplinary team, including a psychiatric, genetic, and reproductive assessment as well as the involvement of an ethics committee. An early diagnosis of DSDs is crucial to avoid the development of potentially serious complications in adulthood.

Experts discuss the case of a 56-year-old white man who presents with multiple immune-related adverse events
Experts discuss the case of a 69-year-old man with a history of metastatic prostate cancer previously treated with androgen deprivation therapy with leuprolide.
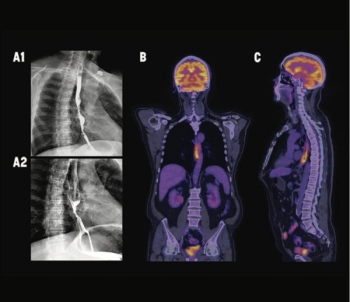
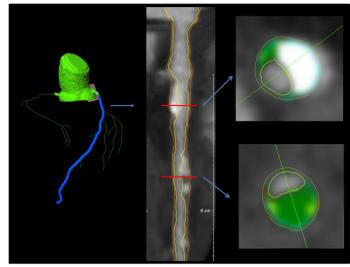
A rare occurrence, cancer in the esophagus requires an individualized treatment plan.
What is the best treatment option after progression to chemotherapy/immunotherapy (chemo/IO) as first-line treatment for PD-L1–positive lung adenocarcinoma with no sensitizing mutations?
Melanoma of the skin is the 19th most common malignant neoplasm worldwide, with 287,723 new cases estimated for 2018 and metastatic melanoma accounting for 4% of all new cases. In recent years, the prognosis of this stage has undergone a dramatic transformation with the advent of immunotherapy and BRAF/MEK targeted therapy.
A 39-year-old woman with no significant medical history presented to the emergency department with progressive diffuse abdominal pain, involuntary weight loss, anemic syndrome, and limitation of mobility. What is the best treatment course to follow?
A 65-year-old man presented with locally advanced, high-risk prostate cancer. His medical history was remarkable for type 2 diabetes mellitus, and he was an active smoker with a 27 pack-year history.
A 67-year-old man, a former smoker, presented with gross hematuria. A CT urogram showed a bladder tumor in the anterior wall and multiple enlarged retroperitoneal lymph nodes. Two vertebral metastases were seen on a bone scan. He underwent a transurethral resection of the bladder, and the pathology report revealed muscle-invasive urothelial carcinoma.
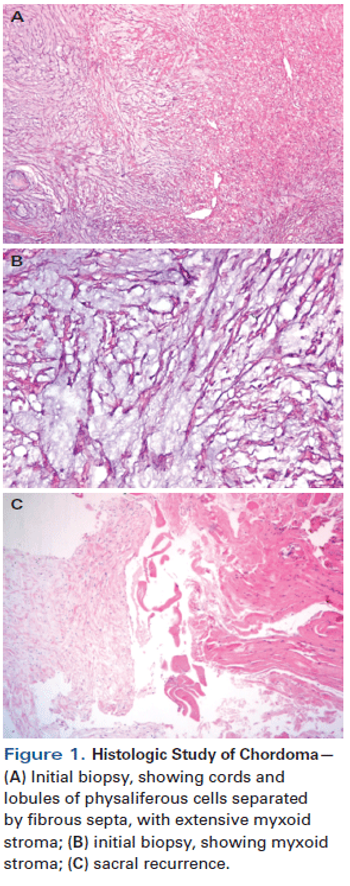
A 60-year-old man presented with lower limb claudication and a painful mass on his left buttock. Physical examination revealed a firm round mass, fixed to deep planes. A biopsy was performed and revealed a chordoma.
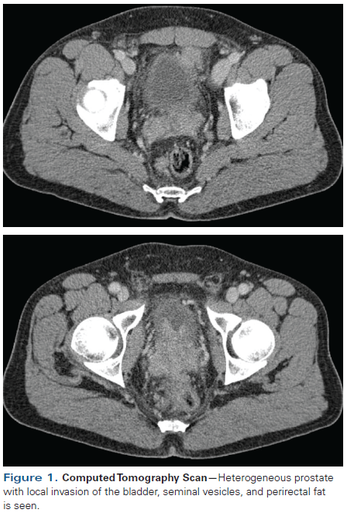
A 55-year-old Hispanic male presents with a family history of gastric cancer in one sibling and prostate cancer in an older brother. CT performed in March 2015 for IMT surveillance showed a heterogeneous prostate with local invasion involving the bladder, seminal vesicles, and perirectal fat.
A 42-year-old man presented with increasing right hip pain that limited his ability to walk. Magnetic resonance imaging (MRI) revealed a right lytic acetabular lesion. Further work-up included a computed tomography (CT) scan, which revealed an 8-cm left kidney tumor.
A 45-year-old man with a known history of rheumatic fever and aortic valve replacement 15 years earlier presented with the chief complaint of a 1-month history of progressive, intense, nonmechanical lumbar pain.
A 63-year-old man with no family history of prostate cancer has prostate biopsy that revealed 9 out of 12 cores involved with prostatic adenocarcinoma, mostly Gleason score 5+4=9.
While evidence points to benefit from highly active hormonal agents in prostate cancer with visceral involvement, the usefulness of immunotherapy is much less clear.
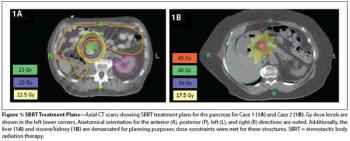
In this edition of our ongoing series, the authors present two cases involving renal cell carcinoma patients treated with SBRT for pancreatic metastases.
A 71-year-old woman presented with back pain and was incidentally found to have a left upper pole renal mass. She underwent left open partial nephrectomy; the pathology results revealed a 2.2-cm clear-cell renal cell carcinoma (RCC) with negative margins and a Fuhrman nuclear grade of 2.

October 14th 2020

October 22nd 2024
April 15th 2022


