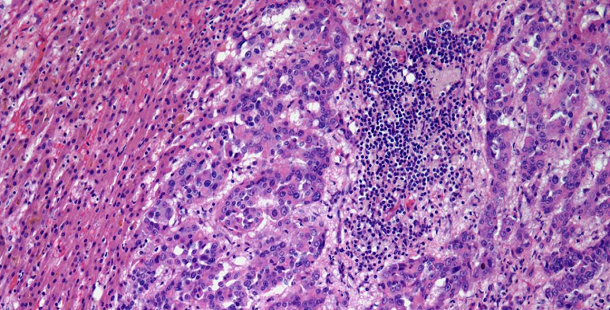





















































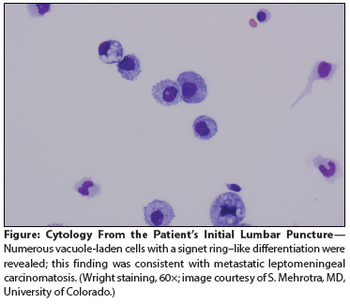
A 59-year-old man with metastatic gastric cancer presented to the oncology clinic with a 1-week history of positional headache, nausea, and vomiting. He stated that the headache was located in the frontal region, was 8 on a scale of 10 in intensity.
A 59-year-old man with metastatic gastric cancer presented to the oncology clinic with a 1-week history of positional headache, nausea, and vomiting. He stated that the headache was located in the frontal region, was 8 on a scale of 10 in intensity.
According to a large study, men with a CDH1 gene mutation have a 70% incidence of gastric cancer by the age of 80 years and women have a 56% incidence.
Adding radiotherapy to adjuvant chemotherapy in the ARTIST trial yielded similar results to chemo alone in patients with D2 lymph node-resected gastric cancer.

The FDA approved ramucirumab (Cyramza) in combination with paclitaxel for treating patients with advanced gastric or gastroesophageal junction adenocarcinoma.

In 2008, 770,000 out of 989,000 gastric cancer cases worldwide were attributed to H pylori, suggesting eradication could yield drastic reductions in incidence.
Expression of the protein ALDH1A1 is associated with outcomes in gastric cancer, according to a new study, and could be used as a prognostic tool.

In a preliminary study using a mouse model, researchers found that vagal denervation using Botox or other methods could help slow gastric cancer’s growth.
A new study from The Cancer Genome Atlas proposes a new classification of gastric cancers into four genomic subtypes that could eventually yield better treatment paradigms.

Searching for and eradicating the bacteria Helicobacter pylori could reduce the incidence of gastric cancer in otherwise healthy individuals, especially in Asian populations, according to a new study.
Both esophageal cancer and stomach cancer are aggressive malignancies with contrasting risk factors, histologies, and molecular characteristics-yet for the most part comparable therapeutic approaches.
The purpose of this review is to update, present some of the new data on, and outline the controversies regarding neoadjuvant and adjuvant therapy of esophagogastric junction and gastric adenocarcinoma.
Adding ramucirumab to FOLFOX did not delay progression in patients with untreated advanced gastric or esophageal adenocarcinoma, according to trial results presented at the 2014 ASCO Annual Meeting.
The VEGFR-2 tyrosine kinase inhibitor apatinib significantly prolonged overall survival in patients with advanced gastric cancer compared with placebo, according to the results of a phase III study.
The FDA has approved the angiogenesis inhibitor ramucirumab for the treatment of gastric cancer and gastroesophageal junction adenocarcinoma.
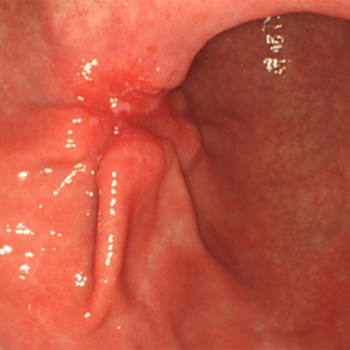
Confocal laser endomicroscopy, a new technology that permits high-resolution subsurface microscopic imaging of living tissue during routine endoscopy, can facilitate the diagnosis of esophageal and gastric cancers, according to a recent report. "Endomicroscopy allows you to make an in vivo histology during ongoing endoscopy," Ralf Kiesslich, MD, PhD, said at the 2006 Gastrointestinal Cancers Symposium (General Session I).
The FDA has approved the use of Taxotere (docetaxel, Sanofi-Aventis) in combination with cisplatin and fluorouracil (5-FU) for the treatment of advanced gastric cancer, including cancer of the gastroesophageal junction, in patients who have not received prior chemotherapy for their advanced disease.
ORLANDO-Chemotherapy given before and after surgery is better than surgery alone for operable gastric and lower esophageal cancers, David Cunningham, MD, reported (abstract 4001).
BEIJING, CHINA-“Capecitabine (Xeloda) plus cisplatin is highly active and well tolerated as first-line treatment of Chinese patients with advanced gastric cancer, with an overall
The 30 reports in this special supplement to Oncology News International represent highlights of ongoing major clinical trials and new research presented at ASCO 2004 regarding state-of-the-art chemotherapeutic management of gastrointestinal and other cancers. Important developments in capecitabine as adjuvant therapy, novel targeted agents, and new combinations are discussed.
This special “annual highlights” supplement to Oncology News International is a compilation of some of the major advances in the management of gastrointestinal cancers during 2003–2004, as reported in ONI. Guest editor Dr. James L. Abbruzzese comments on the reports included herein and discusses advances in the clinical management of GI cancers, with a focus on developments in targeted therapy, new combinations, adjuvant therapy, and what to watch for in 2004.
Docetaxel (Taxotere) has been successfully investigated in the therapy for advanced gastroesophageal tumors as both a single agent and in combination regimens. As a single agent, phase II study results demonstrate an overall response rate of 17% to 24%, with occasional complete responses in a disease in which complete responses are rare. These figures classify docetaxel among the most active agents for the disease.
We conducted a phase II study to assess the response rate and toxicity profile of the irinotecan (CPT-11, Camptosar) plus cisplatin combination administered weekly to patients with at least one previous chemotherapy for advanced adenocarcinoma of the stomach or gastroesophageal junction. Patients with histologic proof of adenocarcinoma of the stomach or gastroesophageal junction with adequate liver, kidney, and bone marrow functions were treated with 50 mg/m² of irinotecan plus 30 mg/m² of cisplatin, both administered intravenously 1 day a week for 4 consecutive weeks, followed by a 2-week recovery period.
Metastatic gastric cancer is a relatively chemosensitive disease. With current regimens, 25% to 40% of patients can be expected to respond, and median survival of 6 to 8 months is
Chemotherapy for advanced gastric and gastroesophageal junction carcinomas remains suboptimal. Both irinotecan (Camptosar) and cisplatin (Platinol) are active against this group of malignancies. This article focuses