
















































































The combination of idelalisib with rituximab improved survival in relapsed CLL, and idelalisib also showed antitumor activity as a single agent in patients with indolent non-Hodgkin lymphoma.
The combination of idelalisib with rituximab improved survival in relapsed CLL, and idelalisib also showed antitumor activity as a single agent in patients with indolent non-Hodgkin lymphoma.
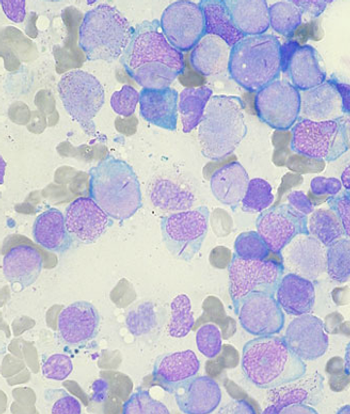
Activating mutations in the beta-catenin gene in bone cells is shown to contribute to the development of acute myeloid leukemia.
After significant improvement in progression-free survival with ibrutinib over ofatumumab, an independent data monitoring board has recommended stopping a phase III trial involving patients with relapsed or refractory CLL or SLL.
In a new study, combining the anti-CD20 antibody obinutuzumab with chlorambucil improved outcomes over rituximab and the same agent in chronic lymphocytic leukemia patients with coexisting conditions.
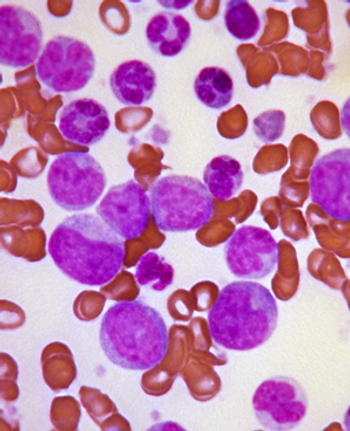
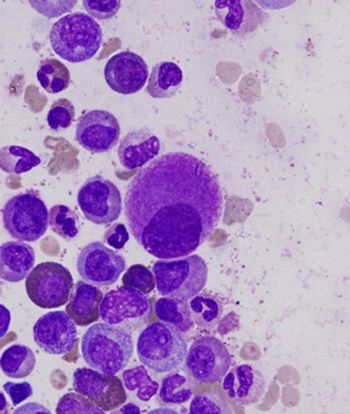
Most physicians are less aware of clinical presentations of the various heavy chain diseases, due in great part to their low incidence and highly variable clinical course. Heavy chain diseases are rare lymphoproliferative B-cell disorders whose hallmark is the accumulation and secretion of truncated constant heavy chains without the associated light chains.
In the absence of a clear understanding of the underlying biologic heterogeneity, the etiology of the different heavy chain diseases (HCDs) should be taken into consideration when treatment decisions are made. Extrapolation from related conditions, such as aggressive lymphomas (in γ-HCD) and CLL (in μ-HCD), suggests that novel and targeted therapies may be effective in the management of these rare diseases.
No definite guidelines exist for the management of nongastric MALT lymphoma. Retrospective series have included patients treated with different modalities, and excellent cause-specific and overall survival have been demonstrated, independent of the type of treatment adopted.
This review discusses the clinical presentation; epidemiology; laboratory, radiologic, and pathologic features; and treatment options for each of the heavy chain diseases, emphasising the importance of an accurate pathologic diagnosis and correct interpretation of immunologic studies in their identification.
Chronic myeloid leukemia (CML) patients with higher copayments for the tyrosine kinase inhibitor imatinib were more likely to discontinue the drug or be non-adherent, according to a new study.
The International Myeloma Working Group recently released a consensus statement updating recommendations for the management and treatment of patients with multiple myeloma who are not eligible for standard autologous stem-cell transplantation.
Two alternative multiple myeloma plasma cell surface markers have been identified and could be important for subclassification, prognostication, and treatment stratification of patients with multiple myeloma.
A deep molecular response to imatinib, achieved by most chronic myeloid leukemia patients who receive the drug, is predictive of better overall survival, according to a new study.
Modulation of the bone marrow microenvironment with parathyroid hormone may be a feasible way to dramatically reduce counts of leukemia stem cells in chronic myeloid leukemia patients, according to new research in mice.
Mesotheliomas that arise after patients receive radiation therapy for lymphoma have unusual histologic features, and those patients tend to be younger and tend to survive longer than more common asbestos-related mesothelioma patients.
A new phase II trial found that a regimen containing rituximab, gemcitabine, cyclophosphamide, vincristine, and prednisolone is active and reasonably safe in patients with diffuse large B-cell lymphoma and coexisting cardiac disease.

A study aimed at defining the natural history of breast implant-associated anaplastic large-cell lymphoma found that outcomes differ between those cases where the disease is confined within the fibrous capsule surrounding the implant and those where a mass is present in the breast.

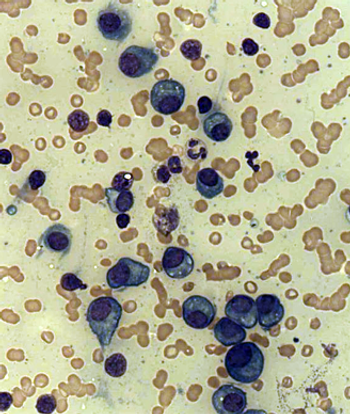
Although the prospect is tempting, we do not believe there are sufficient grounds at this time to abandon bone marrow biopsy in patients with lymphoma. It still provides robust prognostic information, and in the majority of patients it remains an indispensable staging tool.

Clearly, eliminating a bone marrow biopsy in appropriate patients would be another step in the direction of minimizing the torture to which they are subjected.
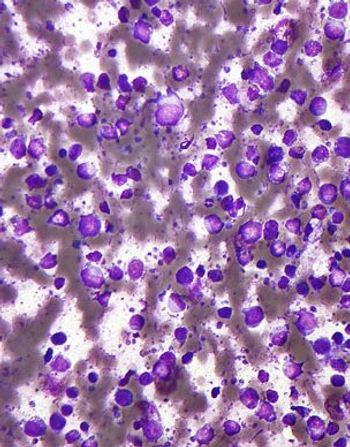
Because of challenges in making the correct diagnosis and the physician’s reluctance to administer chemotherapy for a disease characterized by such a low tumoral mass, patients may experience a delay in the initiation of appropriate treatment.
While the name POEMS (polyneuropathy, organomegaly, endocrinopathy, monoclonal gammopathy, and skin changes) provides a nice acronym for a collection of seemingly disparate features, the diagnosis does not require that all these elements be present, and many other features are not included.
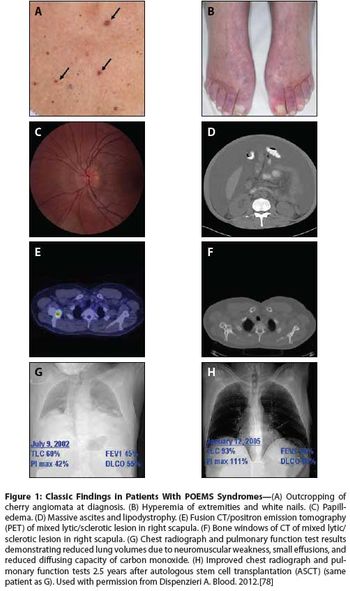
POEMS syndrome is a rare paraneoplastic syndrome that is caused by an underlying plasma cell disorder. Its main features include polyradiculoneuropathy, organomegaly, endocrinopathy, monoclonal plasma cell disorder, and skin changes.
Treatment with gemtuzumab ozogamicin improved the event-free survival in children and adolescents with acute myeloid leukemia by reducing the risk of relapse among those able to achieve remission, according to trial results presented at the 2013 ASH meeting.
Ponatinib showed significant antileukemic activity in patients with CML and ALL, according to a phase II study that included a wide range of disease stages and mutation status; patients in the trial had a relatively high rate of adverse thrombotic events, an issue which has led to recent regulatory controversy surrounding the drug.
Following recent trial data showing an increased risk of dangerous blood clots with ponatinib, which led the FDA to request that the manufacturer stop marketing the drug, the FDA’s European counterpart has adjusted its recommendations for ponatinib but has not changed its “positive opinion” that led to the approval.
This article reviews the etiology and incidence of renal adverse events in patients with multiple myeloma, the renal safety profile of single-agent carfilzomib from four phase II studies in patients with relapsed and/or refractory multiple myeloma, and the management of patients with multiple myeloma who receive carfilzomib and are at risk for renal complications.