






















































Canadian researchers also find that patients are not having recommended cancer screening studies done on a regular basis.
Lymphoma
Latest News
December 6th 2010
Dose-escalated BEACOPP should become new standard of care for early unfavorable Hodgkin’s lymphoma
By Fran Lowry
Advertisement
Advertisement

Here we present the case of a 3-year-old girl with generalized lymphadenopathy and fever, in whom the cause of the symptoms was initially thought to be infectious. Ultimately, however, anaplastic large cell lymphoma (ALCL) was diagnosed. Using this case as a backdrop, we discuss the wide range of systemic illnesses that the differential diagnosis of generalized lymphadenopathy encompasses.
Bruce Cheson, MD, has become chair of the Lymphoma Research Foundation Scientific Advisory Board. Dr. Cheson is professor of medicine, head of hematology, and director of hematology research at the Lombardi Comprehensive Cancer Center at Georgetown University Hospital in Washington DC. His two-year term as chair began in July 2010.
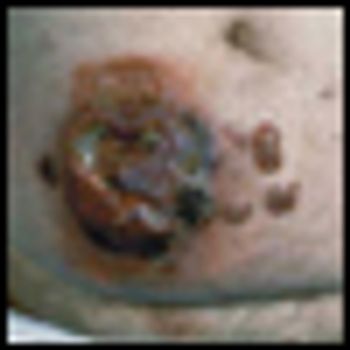
Anaplastic large cell lymphoma (ALCL) is a biologic and clinically heterogenous subtype of T-cell lymphoma. Clinically, ALCL may present as localized (primary) cutaneous disease or widespread systemic disease. These two forms of ALCL are distinct entities with different clinical and biologic features. Both types share similar histology, however, with cohesive sheets of large lymphoid cells expressing the Ki-1 (CD30) molecule. Primary cutaneous ALCL (C-ALCL) is part of the spectrum of CD30+ lymphoproliferative diseases of the skin including lymphomatoid papulosis. Using conservative measures, 5-year disease-free survival rates are>90%. The systemic ALCL type is an aggressive lymphoma that may secondarily involve the skin, in addition to other extranodal sites. Further, systemic ALCL may be divided based on the expression of anaplastic lymphoma kinase (ALK) protein, which is activated most frequently through the nonrandom t(2;5) chromosome translocation, causing the fusion of the nucleophosmin (NPM) gene located at 5q35 to 2p23 encoding the receptor tyrosine kinase ALK. Systemic ALK+ ALCLs have improved prognosis compared with ALK-negative ALCL, although both subtypes warrant treatment with polychemotherapy. Allogeneic and, to a lesser extent, autologous stem cell transplantation play a role in relapsed disease, while the benefit of upfront transplant is not clearly defined. Treatment options for relapsed patients include agents such as pralatrexate (Folotyn) and vinblastine. In addition, a multitude of novel therapeutics are being studied, including anti-CD30 antibodies, histone deacetylase inhibitors, immunomodulatory drugs, proteasome inhibitors, and inhibitors of ALK and its downstream signaling pathways. Continued clinical trial involvement by oncologists and patients is imperative to improve the outcomes for this malignancy.
A multi-institutional group of researchers have zeroed in on a more accurate way to decipher treatment outcomes in young leukemia patients using information from a simple complete blood count test.
Parents and their children need to understand that advancing science does not always go hand-in-hand with a direct benefit to the patients.
Mycosis fungoides (MF), the most common cutaneous T-cell lymphoma, is a low-grade cutaneous lymphoma characterized by skin-homing CD4+ T cells. It is notable for highly symptomatic progressive skin lesions, including patches, plaques, tumors, and erytheroderma, and has a poorer prognosis at later stages. Diagnosis remains difficult owing to MF’s nonspecific skin presentation and identification of the optimal treatment strategy is challenging given the paucity of controlled trials and numerous and emerging treatment options. Management includes topical therapy with the addition of systemic therapy for patients with later-stage disease including tumors; erythroderma; and nodal, visceral, or blood involvement. Topical therapies include mechlorethamine (nitrogen mustard), carmustine (BCNU), steroids, bexarotene gel (Targretin Gel), psoralen plus ultraviolet A (PUVA), ultraviolet B (UVB), and either localized or total skin electron radiotherapy. Systemic therapies include interferon, retinoids, oral bexarotene (Targretin), denileukin diftitox (Ontak), vorinostat (Zolinza), extracorporeal photochemotherapy (photopheresis), and cytotoxic chemotherapy. Herein, we outline clinically relevant aspects of MF, including clinical presentation, pathology, diagnosis, and staging. We describe in detail existing and emerging therapeutics and offer specific recommendations for management of each stage of MF.
The article entitled “Diagnosis and Management of Mycosis Fungoides” by Shira Galper, Benjamin Smith, and Lynn Wilson is an excellent contemporary summary of the workup and management of mycosis fungoides (MF) and its leukemia variant, Sézary syndrome (SS). In their discussion of the diagnosis and staging of MF and SS, the authors include a discussion of proposed revisions by the International Society for Cutaneous Lymphoma and the European Organisation for the Research and Treatment of Cancer (ISCL/EORTC) which seek to identify prognostic subgroups. In addition, there is a complete overview of the various treatment options for management of MF and SS. This treatment overview closely parallels the 2010 National Comprehensive Cancer Network (NCCN) Practice Guidelines for MF and SS.
Galper et al. should be commended for their concise and useful review of the diagnosis and management of mycosis fungoides (MF). It is notable that all of the authors are radiation oncologists. While the reader may expect a radiation oncologist’s perspective on the management of mycosis fungoides, their review goes beyond highlighting the various radiation techniques used in the treatment of MF. It highlights the major diagnostic dilemmas when evaluating patients with skin lesions that eventually are diagnosed as MF or its leukemic counterpart, Sézary syndrome (SS). It also stresses the importance of a multidisciplinary approach in diagnosing and caring for MF patients involving dermatology, dermatopathology, radiation oncology, and hematology/oncology, and provides a concise review of the treatment options in the MF and SS armamentarium. Navigating these options requires a good understanding of the natural history of the disease, the side effects of treatment, the expected response rates of treatment, the median time to response, the patient’s comorbid conditions, and goals of care.

With better disease definition, staging, and monitoring, treatment of extranodal NK/T-cell lymphoma is becoming more rational. A large proportion of patients with localized nasal disease may enjoy prolonged disease-free survival. On the other hand, early HSCT or novel therapy may be recommended for aggressive extranasal disease.
Extranodal natural killer/T-cell lymphoma (ENKTL), nasal type, is a distinct entity of non-Hodgkin lymphoma with interesting unique biologic and clinicopathologic features. The tumor is characterized by ethnic preponderance, a consistent association with Epstein-Barr virus (EBV) infection, peculiar histopathologic findings, and a predilection to affect primarily the upper aerodigestive tract, inclusive anatomically of the nasal cavity, nasopharynx, paranasal sinuses, oral cavity, hypopharynx, and larynx. The characteristic clinical features are nasal stuffiness, relentless, nonhealing ulcers, or symptoms due to obstruction of the aforementioned areas. Distant metastasis at time of diagnosis is uncommon.
Since the creation of the World Health Organization’s nasal natural killer (NK)/T-cell lymphoma category, the attempt to further classify, describe, and improve treatment in this entity has been underway. There has been quite a bit of confusion and frustration regarding diagnosis, staging, and treatment approaches. With his article in this issue of ONCOLOGY, Dr. Au has attempted to improve our knowledge of current approaches to NK/T-cell lymphomas, providing a thorough and contemporary review of the clinical management of these difficult tumors. The following commentary reflects a deep appreciation for the author’s work and expands upon a few points not previously highlighted.
Unlike conventional radiation, Yttrium-90-ibritumomab tiuxetan (Zevalin) induces cellular damage only in the targeted tumor cells and has demonstrated activity in follicular and diffuse large B-cell non-Hodgkin’s lymphoma.
In asymptomatic disease, overall survival is often the same with immediate treatment vs watch and wait. The deciding factor may be what patients are willing to tolerate.
Multiple myeloma remains the second most common hematologic malignancy in the United States, after non-Hodgkin lymphoma.
Hematopoietic malignancies account for 6% to 8% of new cancers diagnosed annually. In the year 2009, an estimated 44,790 new cases of leukemia were diagnosed, and 21,870 deaths were attributable to leukemias of all types. The total age-adjusted incidence of leukemia, including both acute and chronic forms, is 9.6 per 100,000 population; the incidence of acute lymphoblastic leukemia (ALL) is 1.5 per 100,000 and of acute myelogenous leukemia (AML) is 2.7 per 100,000 population.
The incidence rates of non-Hodgkin lymphoma (NHL) in the United States have almost doubled between 1970 and 1990, representing one of the largest increases of any cancer. Although the overall incidence rates of NHL began to stabilize in the late 1990s, the temporal trends varied by histologic subtype. Some of this increase may be artifactual, resulting from improved diagnostic techniques and access to medical care, or directly related to the development of NHL in 25- to 54-year-old men with human immunodeficiency virus (HIV) infection. However, additional factors must be responsible for this unexpected increase in frequency of NHL that has been observed throughout the United States.
In 2009 approximately 8,510 new cases of Hodgkin lymphoma (HL) will be diagnosed in the United States. Over the past 4 decades, advances in radiation therapy and the advent of combination chemotherapy have tripled the cure rate of patients with HL. In 2009, more than 80% of all newly diagnosed patients can expect a normal, disease-free life span.
Induction therapy with higher daily doses of daunorubicin improved complete response and boosted overall survival in younger patients with acute myelogenous leukemia, according to results of the phase III ECOG E1900 trial.
No branch of oncology has been more attuned to the vision of new genetically engineered targeted therapies than the field of hematopoietic malignancies. Ujjani and Cheson have produced a masterful summary of one extremely important component of the targeted therapy revolution-the realm of monoclonal antibodies directed against malignant lymphoma surface antigens.[1] The review presents a wonderful update and a glimpse of future potentially curative macromolecular cocktails. It is an attractive vision.
he treatment of B-cell malignancies has been revolutionized by the availability of safe and effective monoclonal antibodies. The addition of rituximab to standard chemotherapy regimens prolongs the survival of patients with diffuse large B-cell lymphoma (DLBCL) and follicular non-Hodgkin lymphoma. Nevertheless, indolent and mantle cell lymphomas remain incurable, and 30% to 40% of patients with DLBCL still die from their disease. Much ongoing research has focused on optimizing monoclonal antibody use, integrating them into multiagent regimens, and developing newer antibodies. Attempts to improve on the efficacy of monoclonal antibody–based therapy have included altering the dosing schedule, optimizing patient selection, maintenance therapy, improving upon the rituximab molecule, radioimmunotherapy, as well as combinations with cytotoxic molecules and other novel agents. Preliminary data with a number of treatment regimens are promising in indolent and aggressive lymphomas. The eventual goal of targeted therapies is to individualize treatment to increase response and survival, while reducing treatment-related toxicity.
In this review, Ujjani and Cheson present a useful overview of the array of existing and developing roles for monoclonal antibodies in the management of B-cell non-Hodgkin lymphomas (NHLs). These roles may be characterized as single-agent antibody therapy, use in combination with chemotherapy and/or other antibodies, and use following an initial regimen (consolidation/maintenance). Rituximab (Rituxan), the first monoclonal antibody approved for B-cell NHL, clearly has had greatest application in each of these arenas, but it has now been joined by alemtuzumab (Campath) and ofatumumab (Arzerra) as approved single-agent therapies. Also highlighted are a number of other antibodies aimed at B-cell targets: veltuzumab, GA101, AME-133 (CD20), epratuzumab (CD22), lumiliximab (CD23), galiximab (CD80), dacetuzumab (CD40), mapatumumab, lexatumumab (TRAIL), and approaches to improve antibody therapy such as conjugation with radioisotopes or toxins.
Peripheral T-cell lymphomas (PTCLs) are uncommonly encountered malignancies in the United States, and hepatosplenic T-cell lymphoma (HSTCL), subcutaneous panniculitis-like T-cell lymphoma (SPTCL), and enteropathy-type T-cell lymphoma (ETTCL) are rare subtypes of PTCLs that often present with primarily extranodal disease. Despite the fact that these tumors have distinct clinical and pathologic features, they are often diagnosed after significant delay. The combination of delay in diagnosis with ineffective therapies has resulted in a poor prognosis in most cases. Techniques that identify T-cell receptor gene rearrangements and flow cytometry that can identify characteristic immunophenotypes have guided our understanding of the underlying cell of origin of these rare PTCLs. As knowledge regarding the biology of these lymphomas increases alongside the development of newer therapeutics with novel mechanisms, clinicians must accordingly improve their familiarity with the clinical settings in which these rare malignancies arise as well as the pathologic features that make them unique
In this issue of ONCOLOGY, Dr. Tobinai presents a thorough and thoughtful review of the current state of the art of HTLV-related adult T-cell leukemia/lymphoma (ATLL). As described, ATLL is most prevalent in Asia, where it has also been most studied, but is also seen in patients from other HTLV-endemic areas including the Caribbean, South America, and parts of Africa. ATLL is rare in North America and Europe, representing 1% to 2% of T-cell lymphomas compared to 25% in Asia.[1]
In this issue of ONCOLOGY, Tobinai reviews the management of human T-cell lymphotropic virus type 1 (HTLV-1)–associated adult T-cell leukemia/lymphoma (ATL). Although rare in the United States, an estimated 10 to 20 million people are infected with HTLV-1 worldwide and 2% to 5% will develop ATL.[1]
Advertisement
Advertisement
Trending on CancerNetwork
1
177Lu-Edoterotide Handed CRL by FDA For GEP-NETs Treatment
2
BI-1808 Earns FDA Fast Track Status for Advanced Ovarian Cancer
3
DESTINY Trials May Reshape HER2-Positive Breast Cancer Care With T-DXd
4
Bispecific Antibodies for Older Patients With Relapsed/Refractory Multiple Myeloma
5