

Kidney Cancer
Latest News
Advertisement
Latest Videos






















































Advertisement
More News
An external validation study has confirmed that biomarkers of the mTOR pathway have prognostic value in patients with clear cell renal cell carcinoma.
In patients with non–clear cell RCC, PD-L1 positivity is associated with worse clinical outcomes, including a shorter overall survival and time to recurrence.
Results of a new study show that cancer rates among children and adolescents are stable, but rates of certain cancers such as renal carcinomas are increasing.
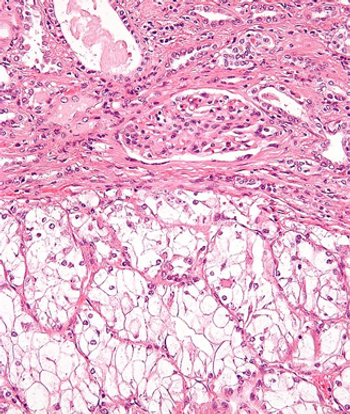
A 71-year-old woman presented with back pain and was incidentally found to have a left upper pole renal mass. She underwent left open partial nephrectomy; the pathology results revealed a 2.2-cm clear-cell renal cell carcinoma (RCC) with negative margins and a Fuhrman nuclear grade of 2.

Patient exposure to metformin before undergoing nephrectomy for renal cell carcinoma may have an effect on patient survival, according to a new study.
Preoperative levels of C-reactive protein may be as predictive of outcomes as pathological TNM stage or tumor grade for prognosis in renal cell carcinoma.

A new study shows yet another link between increasing body mass index (BMI) and the risk of several common cancers, including kidney cancer.
Expression of microRNA (miR)-23b/27b cluster has been linked with increased risk for clear cell RCC disease progression, and may be a predictor of poor survival.
Researchers have identified a key gluconeogenic enzyme, the absence of which in clear cell renal cell carcinoma (RCC) may explain the uncontrolled cell growth present in cancer cells compared with normal kidney cells.
Results of a head-to-head comparison of first-line treatment of metastatic renal cell carcinoma with the mTOR inhibitor everolimus or VEGF inhibitor sunitinib showed that everolimus did not meet noninferiority requirements as a first-line therapy.
Scientists have discovered a new molecular target for therapy to fight clear cell renal cell carcinoma, neuronal pentraxin 2 (NPTX2).
Among patients with clear cell renal cell carcinoma who had undergone nephrectomy, patients with diabetes were found to have a significantly decreased cancer-specific and overall survival.
A 16-gene Recurrence Score was found to be significantly predictive of recurrence-free interval and survival in patients with stage I-III clear cell renal cell carcinoma who have undergone nephrectomy.

Patients with renal cell carcinoma who had low preoperative levels of serum cholesterol were found to have worse survival, according to the results of a recent study.
While seven drugs have been approved for clear cell renal cell carcinoma (ccRCC) since 2005, the most appropriate systemic therapy for non-clear cell renal cell carcinoma (nccRCC) is unknown.

A reduced estimated glomerular filtration rate (eGFR) was found to be associated with a significantly increased risk for renal and urothelial cancer, according to the results of a recently published study.
High-dose interleukin-2 remains an important treatment for patients with metastatic renal cell carcinoma, producing durable responses even in those patients with chronic renal insufficiency, according to a recent study.
Results from two large cohorts indicated that increasing blood pressure levels were associated with an increased risk for developing kidney cancer among both men and women.
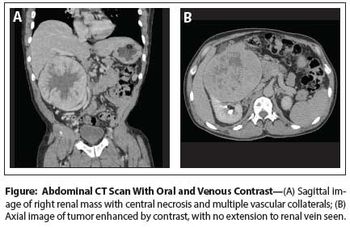
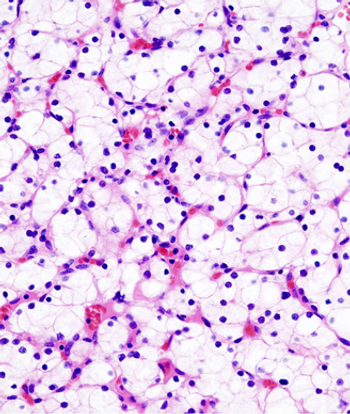
Case History: 60-year-old man with mild right side abdominal discomfort and hepatomegaly found to have large right renal mass during CT scan.
A study of patient preference revealed that patients who participated in a crossover trial of pazopanib and sunitinib for metastatic renal cell carcinoma preferred treatment with pazopanib.
Patients receiving treatment with sunitinib for advanced renal cell carcinoma experienced worse treatment-related fatigue during the first cycle of treatment with symptoms lessening after subsequent consecutive cycles.

A history of significant cigarette smoking adversely affected overall survival in patients who underwent surgery for clear-cell renal cell carcinoma, according to the results of a recent study.
The FGF inhibitor dovitinib failed to improve progression-free survival outcomes as a third-line treatment for patients with metastatic renal cell carcinoma compared with sorafenib, according to the results of a new study.
New research shows that tumors found in obese patients may be more indolent than those in nonobese patients, and this may, in part, be related to alterations in fatty acid metabolism explaining the obesity paradox in clear-cell renal cell carcinoma.

The order of the sequencing of sorafenib and sunitinib for first-line and second-line therapy did not affect progression-free and overall survival for patients with advanced renal cell carcinoma.
Advertisement
Advertisement
Trending on CancerNetwork
1
FDA Approves RP1/Nivolumab for Progression on Anti–PD-1 Therapy in Melanoma
2
The Lowest-Ever Hazard Ratio in Multiple Myeloma Bispecific Trials?
3
Why Earlier CAR T-Cell Therapy May Benefit Patients With Multiple Myeloma
4
Developers Initiate Phase 2/3 Ivonescimab/EV Trial in Bladder Cancer
5