






















































A turning point in therapy followed the observation that patients with AO tumors with chromosome 1p and 19q codeletion had better outcomes when treated with irradiation and PCV than did non-codeleted anaplastic oligodendroglioma patients.
Brain Cancer
Latest News
Advertisement
Advertisement
In light of the high bar that must be met for results to be truly practice-changing, and of the long period of time before survival results are mature in an indolent disease, the primary endpoint for clinical trials in anaplastic oligodendroglial tumors needs rethinking.

Although important questions still remain regarding chemotherapy choice, sequence, and dosing, the answers to which will require additional large phase III trials, radiotherapy alone is no longer appropriate therapy for 1p/19q codeleted anaplastic oligodendrogliomas.
The combination of whole-brain radiation therapy and the EGFR inhibitor erlotinib showed a promising response rate and was well tolerated in a new phase II trial of patients with brain metastases from non-small-cell lung cancer.
Higher levels of the enzyme kallikrein 6 (KLK6) are associated with glioblastoma multiforme, the most common type of brain tumor, according to a new study from researchers at the Mayo Clinic.
Researchers have identified metformin, a drug used to treat diabetes, as a way to activate a key protein that can shut down the continued self-renewal process that keeps producing new glioma cells in glioblastoma patients.
Of particular relevance for clinicians is the possible recommendation of omitting concurrent chemotherapy with CSI in adults, due to the lower marrow reserves and overall lack of data for clear efficacy of concurrent chemotherapy in adults. Additional refinement of these therapeutic regimens for adult medulloblastoma awaits further advances in both the molecular prognostic associations for these tumors and the potentially exciting development of targeted therapies for specific molecular subtypes.
Here we present the history, staging system, and treatment of medulloblastoma, reviewing the prognostic value and clinical application of molecular subtyping while highlighting the differences between adult and pediatric disease.
Future studies of adult medulloblastoma should include whole genome sequencing and identification of the tumorigenic cell origin of adult medulloblastoma. Ultimately, quality prospective trials are needed in adult medulloblastoma patients in order to optimize the management of this rare and complex disease.
A new drug combination of lapatinib (Tykerb) and capecitabine (Xeloda) shrunk brain tumors in HER2-positive breast cancer patients whose cancer had spread to the brain, showing it is active as a first-line brain metastases treatment with similar efficacy to whole-brain radiotherapy.
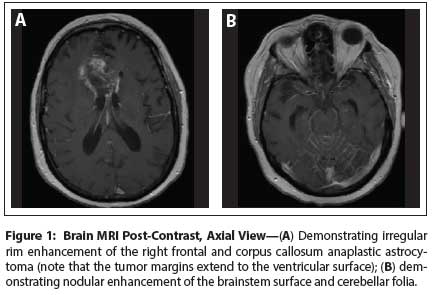
The family of a young woman with a brainstem glioma has been haranguing her physician to continue bevacizumab treatment despite a significant decline in her functional status. How to respond?

The FDA approved a dissolvable form of everolimus (Afinitor Disperz) for the treatment of children with subependymal giant cell astrocytoma (SEGA) that cannot be treated with surgery.
The diagnosis of central nervous system (CNS) recurrence is a much dreaded outcome among breast cancer patients, and its incidence varies with disease stage and cancer subtype.

CancerNetwork speaks with Patricia S. Steeg, PhD, who has recently written a perspective in the journal Nature calling for a shift in both the types of drugs that are developed for breast cancer and in the way clinical trials are designed and executed.
The last two decades have seen the development of a variety of novel therapeutic agents that have improved prognoses for women with breast cancer.
In this issue of ONCOLOGY, Drs. Lim and Lin present a comprehensive and up-to-date review of the basic biology of breast cancer brain metastasis (BCBM) and of emerging strategies for treating this increasingly common complication of advanced breast cancer (BC) (BC is second only to non–small-cell lung cancer in the frequency of central nervous system [CNS] metastasis.)
Results from a phase II clinical trial with HSPPC-96 (vitespen), an autologous heat shock protein-peptide vaccine, have shown promise in patients with recurrent glioblastoma multiforme.
Hypofractionated stereotactic radiotherapy (SRT) appears to be safe and effective in preventing recurrence at resection cavities following surgical resection of brain metastasis and may spare many patients from whole brain radiotherapy (WBRT) and its adverse effects.
Researchers have reported cases of brain tumors among cardiologists and radiologists that work in cardiac catheterization laboratories. In addition to support from the literature, documenting 5 cases of brain tumors, a new study reports 4 new cases of brain malignancies, all in the left hemisphere of the brain.

The US Food and Drug Administration (FDA) has approved a portable noninvasive device, worn on the head, to treat adults whose glioblastoma multiforme (GBM) recurs or progresses following chemotherapy and radiation therapy.
The odds are exceedingly slim that you'll ever see an intracranial MPNST. With no established treatments and tough clinical dilemmas, you don't want to. But 3 recent case reviews and new insights from biology suggest this rare tumor may finally be vulnerable.
Typically glioblastoma patients are dead within 15 months of diagnosis, no matter how complete and well-planned their therapy.
The Ivy Glioblastoma Atlas Project will track genetic mutations in glioblastoma multiforme and produce a free, online medical atlas. The Seattle-based project is a partnership between the Ben and Catherine Ivy Foundation, the Allen Institute for Brain Science, and the Ben and Catherine Ivy Center for Advanced Brain Tumor Treatment at the Swedish Neuroscience Institute.

In July 2009, the US Food and Drug Administration (FDA) granted approval for use of the vascular endothelial growth factor (VEGF) inhibitor bevacizumab (Avastin) in combination with interferon alfa for treatment of patients with metastatic renal cell carcinoma (RCC).
Adult survivors of childhood craniopharyngiomas, the second most common type of childhood brain tumor, face many challenges, including multiple life-threatening metabolic abnormalities. Serious metabolic deficits can result from injury to the pituitary gland or hypothalamus.
Advertisement
Advertisement
Trending on CancerNetwork
1
Epcoritamab Combo Shows Sustained Remissions in Follicular Lymphoma
2
Olomorasib Earns FDA Breakthrough Therapy in KRAS G12C+ Pancreatic Cancer
3
GLP-1 Receptor Agonists and Cancer: Renewed Momentum for Metabo-Oncology
4
Understanding The Training, Credentialing Landscapes for End-of-Life Doulas
5