



























































A recent retrospective study found that adding chemotherapy to postoperative treatment of craniospinal radiation for adults with medulloblastoma improves survival.
A recent retrospective study found that adding chemotherapy to postoperative treatment of craniospinal radiation for adults with medulloblastoma improves survival.
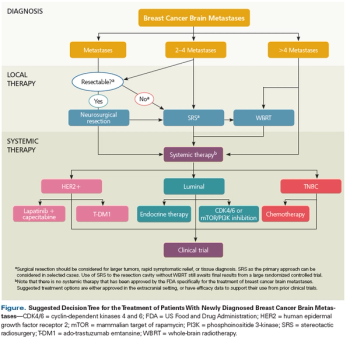
This review summarizes the most up-to-date approach to the multidisciplinary management of patients with breast cancer brain metastases.
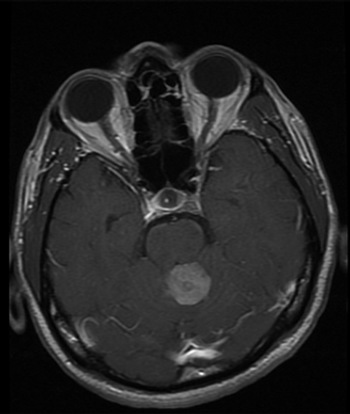
Brain metastasis remains a relatively common and particularly devastating complication of breast cancer and has proven a particularly challenging area for therapeutic innovation.
Use of the targeted therapy dabrafenib resulted in a high overall response rate and was well tolerated in a small phase I/II study of pediatric BRAF V600-mutant low-grade glioma.

A new study is suggesting that radiomic features subjected to machine learning algorithms may be able to identify imaging signatures that defined a subset of patients with recurrent glioblastoma who may gain the most benefit from antiangiogenic therapy.
The use of an intensified treatment regimen to treat metastatic medulloblastoma in children and adolescents conferred an overall favorable survival, according to the results of a recent study. However, patients within varying subgroups and with certain biologic parameters did not have uniform outcomes.
In children with primary brain tumors who were treated with cranial radiation, cerebral volume and radiation dose may affect the rate of vocabulary development.
Vinblastine monotherapy produced outcomes similar to current therapies in children with treatment-naive pediatric low-grade glioma, and had favorable toxicity and quality-of-life profiles.
The deferral of postoperative radiotherapy is increasing among children with medulloblastoma, and this deferral of treatment was associated with worse survival.
Patients with different molecular subtypes of medulloblastoma, a common type of childhood brain tumor, have varying decline in brain function following radiation therapy for their disease.
Patients with glioblastoma who were uninsured or who had Medicaid at the time of diagnosis were more likely to be diagnosed with a larger tumor and had shorter survival times.
The underexpression of one of the homeobox (HOX) genes, HOXA11, is associated with poor prognosis in patients with glioblastoma.

In this video we discuss the use of concurrent immunotherapy and stereotactic radiosurgery for treatment of melanoma brain metastases.
Undergoing immunotherapy within a month of stereotactic radiosurgery resulted in an improved response to treatment for patients with melanoma brain metastases.

Adjuvant temozolomide chemotherapy following radiotherapy improves survival among patients with anaplastic gliomas that do not harbor 1p/19q co-deletions, according to interim results from a phase III trial.
Combined temozolomide and radiotherapy offer significantly better overall survival than radiotherapy alone in patients with glioblastoma multiforme (GBM) who undergo biopsy only rather than surgical resection.
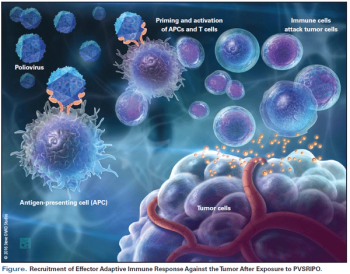
The US Food and Drug Administration granted the “breakthrough therapy” designation to a recombination poliovirus/rhinovirus conjugate known as PVS-RIPO, for treatment of recurrent glioblastoma multiforme.

This review will discuss examples of clinical applications of tumor and germline genomic testing for children with central nervous system (CNS) tumors, as well as promising investigative strategies.
One recurring theme from genomic studies of pediatric CNS tumors (and almost all cancers, for that matter) is that tumors that historically appeared to be a single entity based on examination under the microscope and routine immunohistochemical staining actually harbor molecularly distinct subgroups when analyzed by genomic sequencing techniques.

The aggressive management of brain metastases with SRS has supplanted radiation therapy in an effort to maintain patient quality of life in an era of advancing systemic cancer options.

Until prospective randomized clinical data accrue and mature, this controversial issue will continue to suffer from overinterpretation of inadequate supporting data.
The combination of chemotherapy and radiation therapy resulted in longer overall survival than radiation alone in certain patients with grade 2 gliomas, according to long-term results from a randomized trial.
First-line crizotinib therapy offered better intracranial disease control rate than chemotherapy in patients with ALK-positive non–small-cell lung cancer (NSCLC) and stable treated brain metastases.
In this article, we will discuss some of the vaccination and oncolytic virus strategies being evaluated in the clinic for malignant gliomas. The vaccines reviewed here include the cell-based and the non–cell-based.
The promise of vaccine-based anticancer therapies has been explored for a number of years. However, the research met with little success in its early phases, largely because of a poor understanding of the biology of the immune system and its role in combatting cancer.