












































































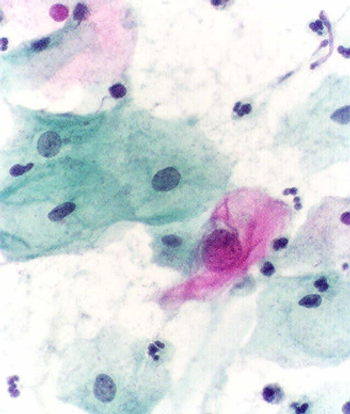
More than 11% of all eligible women had not been screened for cervical cancer in the past 5 years, according to a study by researchers at the CDC.
More than 11% of all eligible women had not been screened for cervical cancer in the past 5 years, according to a study by researchers at the CDC.

Researchers are estimating that about 3.6% of new cancer cases in 2012 in adults may be attributed to a high BMI, equating to about 481,000 new cancer cases.
Nurses trained in the visual inspection with acetic acid cervical cancer screening method were able to successfully perform colposcopy and detect cervical lesions.
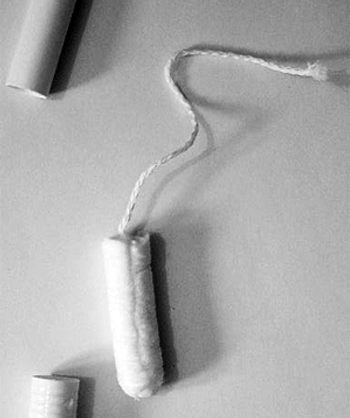
Ovarian cancer cells were detected by collecting and testing DNA specimens taken from the tampons of ovarian cancer patients prior to surgery for a pelvic mass.

Vaccines including that for HPV, which helps prevent cervical cancer, show no association at all with multiple sclerosis or other CNS demyelinating syndromes.
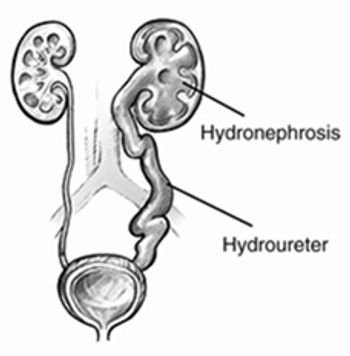
Hydronephrosis is associated with substantial morbidity in patients with cervical cancer, and is potentially associated with poorer survival as well.

Women with an overall higher quality diet prior to diagnosis with ovarian cancer may have a lower risk of all-cause mortality, according to a new study.

A new human papillomavirus (HPV) vaccine that protects against nine types of HPV and would protect against about 90% of cervical cancers could be available in 2015.
Adding the TKI cediranib to chemotherapy improved progression-free survival in patients with metastatic or relapsed cervical cancer, according to a study presented at the 2014 ESMO Congress.

The US Food and Drug Administration has approved bevacizumab (Avastin) for the treatment of patients with recurrent or metastatic cervical cancer.

Researchers found that uterine cancers were present in 27 per 10,000 women undergoing morcellation, which fragments the uterus and can spread cancer cells.

In light of the recent FDA approval of HPV testing for women as a screening method for cervical cancer, we discuss changing guidelines with two experts.
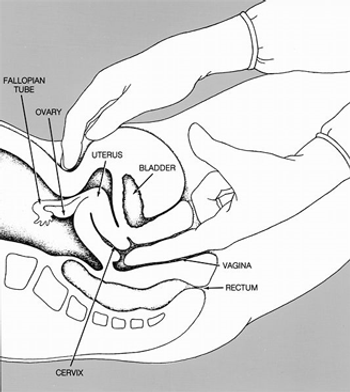
A new clinical practice guideline from the American College of Physicians recommends against conducting routine pelvic exams in average-risk, asymptomatic women.
A new guide developed by nurses and patients with gynecologic cancer offers a much-needed practical resource for women struggling to understand the impact of cancer treatment on their sexual health.

The University of North Carolina has multiple posters accepted to the Gynecologic Oncology General Poster Session at this year’s ASCO meeting. Let’s take a virtual walk through several of these abstracts.
In this interview we discuss the diagnosis and treatment of endometrial cancer, a gynecologic cancer that forms in the tissue lining the uterus.
The FDA has approved an HPV DNA test to be used as a primary screening method for cervical cancer in women 25 and older. The test can also give insight into future risk of cervical cancer.
An FDA panel has recommended that a DNA test that screens for HPV in women can replace the standard Pap smear as a first-line primary cervical cancer screening test.

The Society of Gynecologic Oncology (SGO) recently issued two new clinical practice statements recommending genetic testing for all women with endometrial and ovarian cancers, regardless of family history.
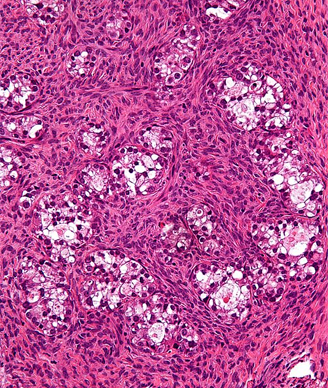
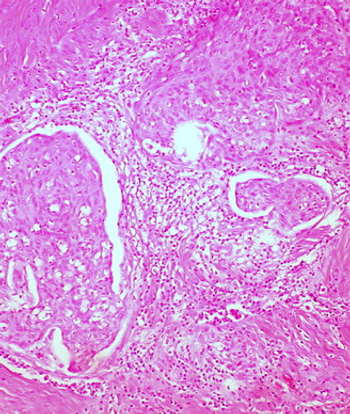
A 71-year-old woman not on hormone replacement therapy presented with uterine bleeding. Dilation and curettage revealed complex hyperplasia with atypia, focal clear-cell features, and endocervicitis. Endometrial intraepithelial carcinoma was suspected.
A new study found that high concentrations of vitamin C increased the effectiveness of chemotherapy in an ovarian cancer mouse model. A high-dose delivery of the vitamin also resulted in lesser toxicity from chemotherapy in cancer patients.
A new study has demonstrated that a therapeutic vaccine against HPV can stimulate an immune response and regression of high-grade cervical dysplasia, a precursor to cervical cancer in women with an HPV infection.